INTRODUCTION
Lymphoma is a type of solid tumor, which develops in immune system and consists of Hodgkin lymphoma and non-Hodgkin lymphoma (NHL) and NHL accounts for 90% of lymphomas [1]. According to World Health Organization (WHO) classification, adult NHL can be divided into B-cell lymphoma or T-cell and natural killer cell lymphoma subtypes based on its origination [2]. Diffuse large B-cell lymphoma is the most typical type among over 80 unique forms of NHL [2]. Its incidence rate has been constantly increasing in many regions around the world [3, 4]. In 2013, NHL has an estimation of 71,850 new cases of incidence and 19,790 deaths in USA, which ranked 8th in invasive cancer incidence rates [3]. The incidence of NHL might associate with several risk factors, including age, gender, infectious agents (such as HIV and Epstein-Barr virus), chemicals, medical treatments, genetic background and autoimmune diseases [5]. Meanwhile, its wide range of clinical features and histological appearances at presentation led to its complication in diagnosis [1].
Along with the advanced biological understanding and improved treatments of NHL, several curative strategies were proposed for the management of this malignance disease [6]. The common treatments for NHL included chemotherapy, radiotherapy, immunotherapy, antibiotic therapy, stem cell transplantation and surgery, depending on the disease type, stage (defined as stage I-IV) and health condition of patient [1]. Among the treatments, radiotherapy had been found to be highly effective to many types of lymphoma, while chemotherapy had been identified as a reliable and effective approach for treating advanced or aggressive NHL.
Combinations of several drugs including rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone, methotrexate and etoposide were often used in chemotherapeutic regimens [7]. CHOP had been developed as the first-generation chemotherapy regimen consisting of doxorubicin, cyclophosphamide, prednisone, and vincristine, which had the potential to cure approximately 30% of NHL patients in advanced stage [8]. Later, on the basis of CHOP, several second or third-generation regimens had been developed, such as increasing fractional dose of CHOP (I-CHOP), incorporating with new and active drugs (i.e. ProMACE-CytaBOM, MACOP-B) and combining the drugs with antiretroviral therapy or immunotherapy (i.e. CHOP-HARRT, R-CHOP) The addition of anti-CD20 monoclonal antibody rituximab to CHOP (R-CHOP), approved by FDA (Food and Drug Administration) in 1997, it had been adapted as a standard regimen to treat newly diagnosed diffuse large B-cell NHL in revised International Prognostic Index [9, 10].
However despite the availability of multi-agent chemotherapy and other types of therapies, few efforts were made to assess the current evidence to obtain the optimum treatment. The relative effectiveness and safety of interventions still remain unclear. For example, although CHOP and R-CHOP had both been commonly adopted in NHL clinical treatments, some studies suggested that R-CHOP could significantly reduce the risk of treatment failure [11] and improve OS among patients [12] while another study implied that rituximab did not improve clinical outcomes [13]. Besides, randomized controlled trials (RCTs) and current published meta-analyses mainly focused on the pair-wise comparisons, such as comparison of CHOP versus R-CHOP [14], GM-CSF versus CHOP [6], and third generation MACOP-B or m-BACOD or ProMACE-CytaBOM versus CHOP [15], etc. Although the evidence supported the efficacy of these treatments, no network meta-analysis (NMA) was reported to compare the therapeutic efficacy among different regimens. For the purpose of compensating the lack of head-to-head comparison, and providing additional evidence about the contradiction mentioned above, this NMA was conducted to integrate current MA and RCTs based on several response and prognostic outcomes. Moreover, we reasonably ranked those treatments to further evaluate the different efficacy of chemotherapies for the benefit of NHL patients.
RESULTS
Characteristics of included studies
First of all, 1,979 publications were identified according to the abovementioned searching strategy. Secondly, 445 duplicated records were removed, then, 1,321 and 199 records were further excluded after abstract and full-text screening because of the different focus, lack of proper comparison or shortage of prognostics data. Through thorough assessment of eligibility, eventually 14 studies published from 1992 to 2009 complied with the criteria and a total of 4,167 patients were included in this NMA [11, 13, 16-27]. Flow chart demonstrating selection process was shown in Figure 1. The baseline characteristics of each study were presented in Table 1, and details specific to each treatment were described in Supplementary Table 1. Network diagram of treatments included in quantitative analysis was shown in Figure 2. For every pair-wise comparison, there was only one study included, except for the comparison between R-CHOP and CHOP which included two studies.
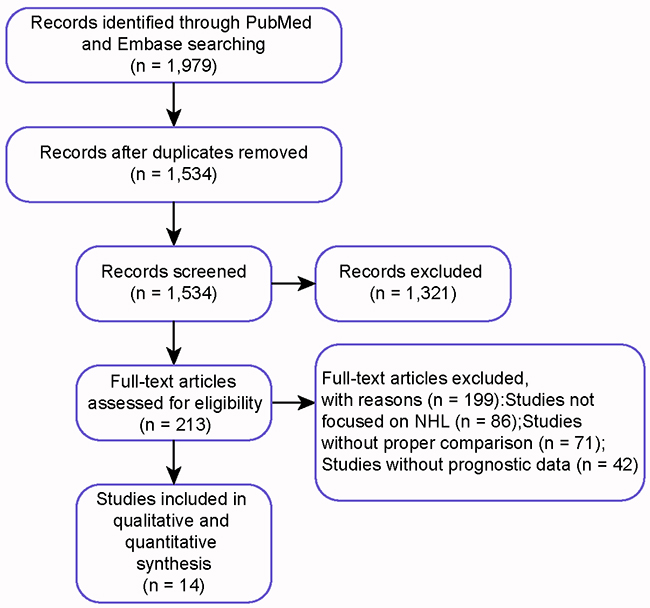
Figure 1: PRIMSA flow chart.
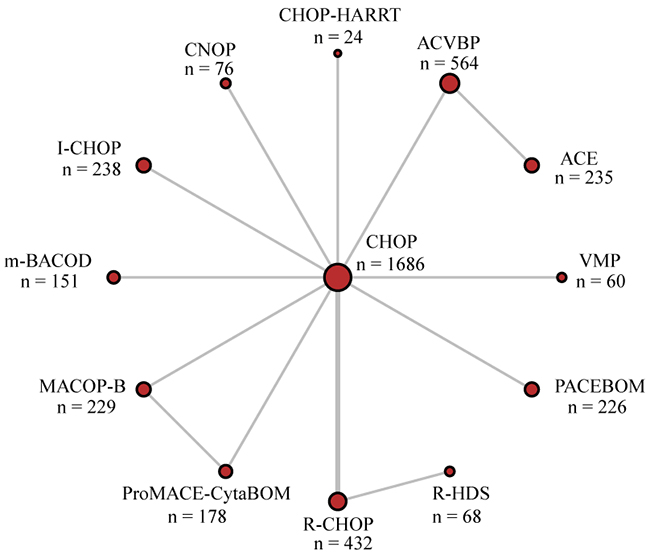
Figure 2: Network diagram of trials included in quantitative analysis. Each node represents a treatment type; lines between two nodes represent direct comparison of these two treatments.
Table 1: Patient parameters of included studies
Author |
Year |
Country |
Follow-up* |
Treatment** |
N |
M/F |
Age*** |
Disease Stage |
|
|---|---|---|---|---|---|---|---|---|---|
I-II |
III-IV |
||||||||
Haioun |
2009 |
France |
72 |
ACVBP |
241 |
287/189 |
48 (18, 60) |
NA |
NA |
ACE |
235 |
NA |
NA |
NA |
NA |
||||
Ladetto |
2008 |
Canada |
80 |
R-CHOP |
66 |
40/26 |
51 (22, 59) |
NA |
NA |
R-HDS |
68 |
38/30 |
51 (25, 59) |
NA |
NA |
||||
Verdonck |
2007 |
Netherlands |
72 |
CHOP |
239 |
135/104 |
50 (16, 65) |
44 |
114 |
CHOP-G-CSF |
238 |
133/105 |
50 (16, 65) |
32 |
206 |
||||
Habermann |
2006 |
USA |
60 |
R-CHOP |
267 |
139/128 |
69 (60, 92) |
25 |
75 |
CHOP |
279 |
134/145 |
70 (60, 92) |
27 |
73 |
||||
Kaplan |
2005 |
USA |
36 |
R-CHOP |
99 |
65/34 |
43 (26, 69) |
0 |
79 |
CHOP |
50 |
29/21 |
40 (26, 73) |
0 |
40 |
||||
Tilly |
2003 |
France |
108 |
ACVBP |
323 |
182/141 |
65 |
56 |
267 |
CHOP |
312 |
177/135 |
65 |
59 |
253 |
||||
Vaccher |
2001 |
Italy |
70 |
CHOP-HARRT |
24 |
20/4 |
38 |
7 |
17 |
CHOP |
80 |
68/12 |
37 |
20 |
60 |
||||
Linch |
2000 |
UK |
144 |
CHOP |
233 |
NA |
NA |
NA |
NA |
PACEBOM |
226 |
NA |
NA |
NA |
NA |
||||
Tirelli |
1998 |
Netherlands |
60 |
VMP |
60 |
NA |
NA |
NA |
NA |
CHOP |
60 |
NA |
NA |
NA |
NA |
||||
Wolf |
1997 |
Australia |
60 |
MACOP-B |
125 |
NA |
NA |
NA |
NA |
CHOP |
111 |
NA |
NA |
NA |
NA |
||||
Montserrat |
1996 |
Spain |
72 |
CHOP |
76 |
31/45 |
NA |
22 |
54 |
ProMACE-CytaBOM |
72 |
45/24 |
NA |
16 |
56 |
||||
Sonneveld |
1995 |
Netherlands |
60 |
CNOP |
76 |
34/40 |
71 (60, 84) |
13 |
63 |
CHOP |
72 |
42/32 |
70 (60, 82) |
15 |
57 |
||||
Silingardi |
1995 |
Italy |
48 |
ProMACE-CytaBOM |
106 |
49/57 |
NA |
36 |
70 |
MACOP-B |
104 |
38/66 |
NA |
37 |
65 |
||||
Gordon |
1992 |
USA |
48 |
CHOP |
174 |
95/79 |
NA |
0 |
174 |
m-BACOD |
151 |
81/70 |
NA |
0 |
151 |
||||
* Follow-up, month.
** Treatment, further description of each treatment can be seen in Supplementary Table 1.
*** Age, mean (range).
OS results from NMA
In order to evaluate the prognostic survival result of each treatment, HRs with 95% CrIs were compared in the NMA presented in Table 2. In the outcome of 1-year OS, no significant difference stood out from the comparison. However, in terms of 2-year, 3-year and 5-year OS, patients of CNOP exhibited the least favorable results compared to other treatments. It indicated the poor long-term prognostic outcomes in CNOP treated patients. Moreover, we observed significant advantages of R-CHOP treatment over CHOP (HR=0.70; 95% CrIs=0.51-1.04) and VMP (HR=0.46; 95% CrIs=0.21-0.98) in view of 3-year OS, indicating R-CHOP as a more effective treatment. As the majority of included studies were based on the comparison with CHOP, forest plots were also conducted to visually elucidate the OS differences between CHOP and other treatments in Figure 3. It had shown significantly lower efficacy of CNOP in 2-year OS (HR=1.68, 95% CrIs=1.01-2.80), 3-year OS (HR=1.69; 95% CrIs=1.06-2.72) and 5-year OS (HR=1.75; 95% CrIs=1.15-2.68) results, and significantly increased 3-year OS in R-CHOP patients when compared to CHOP (HR=0.70; 95% CrIs=0.51-0.96).
Table 2: 1-year to 5-year overall survival of non-Hodgkin lymphoma treatments
CHOP |
0.88 (0.60, 1.30) |
0.87 (0.67, 1.14) |
1.01 (0.44, 2.35) |
1.68 (1.01, 2.80) |
0.75 (0.44, 1.26) |
0.89 (0.59, 1.35) |
0.84 (0.53, 1.34) |
0.89 (0.62, 1.29) |
0.78 (0.46, 1.33) |
0.96 (0.61, 1.51) |
1.13 (0.21, 6.15) |
1.51 (0.73, 3.10) |
||
0.89 (0.39, 2.07) |
ACE |
0.99 (0.75, 1.32) |
1.15 (0.46, 2.91) |
1.91 (1.01, 3.63) |
0.85 (0.44, 1.62) |
1.01 (0.57, 1.79) |
0.96 (0.52, 1.76) |
1.02 (0.59, 1.74) |
0.89 (0.46, 1.72) |
1.09 (0.60, 1.99) |
1.29 (0.23, 7.31) |
1.72 (0.76, 3.89) |
||
0.92 (0.51, 1.67) |
1.03 (0.57, 1.87) |
ACVBP |
1.16 (0.48, 2.81) |
1.93 (1.09, 3.42) |
0.86 (0.48, 1.53) |
1.02 (0.62, 1.67) |
0.97 (0.57, 1.65) |
1.02 (0.65, 1.61) |
0.90 (0.50, 1.62) |
1.10 (0.65, 1.86) |
1.30 (0.23, 7.20) |
1.73 (0.80, 3.73) |
||
0.93 (0.31, 2.77) |
1.04 (0.26, 4.11) |
1.00 (0.29, 3.49) |
CHOP-HARRT |
1.66 (0.62, 4.42) |
0.73 (0.27, 1.97) |
0.88 (0.34, 2.24) |
0.83 (0.32, 2.17) |
0.88 (0.35, 2.20) |
0.77 (0.29, 2.08) |
0.95 (0.36, 2.46) |
1.12 (0.17, 7.38) |
1.49 (0.49, 4.49) |
||
1.79 (0.80, 3.99) |
2.00 (0.63, 6.39) |
1.94 (0.71, 5.26) |
1.93 (0.50, 7.50) |
CNOP |
0.44 (0.21, 0.92) |
0.53 (0.27, 1.02) |
0.50 (0.25, 1.00) |
0.53 (0.28, 1.00) |
0.47 (0.22, 0.97) |
0.57 (0.29, 1.13) |
0.67 (0.11, 3.94) |
0.90 (0.37, 2.17) |
||
0.83 (0.34, 2.02) |
0.93 (0.27, 3.15) |
0.90 (0.31, 2.62) |
0.89 (0.22, 3.67) |
0.46 (0.14, 1.54) |
I-CHOP |
1.19 (0.61, 2.33) |
1.13 (0.56, 2.28) |
1.20 (0.63, 2.27) |
1.05 (0.50, 2.21) |
1.29 (0.65, 2.57) |
1.52 (0.26, 8.92) |
2.02 (0.83, 4.93) |
||
1- OS |
0.90 (0.42, 1.94) |
1.01 (0.32, 3.14) |
0.97 (0.37, 2.58) |
0.97 (0.25, 3.70) |
0.50 (0.17, 1.53) |
1.09 (0.33, 3.53) |
m-BACOD |
0.95 (0.51, 1.77) |
1.00 (0.57, 1.75) |
0.88 (0.45, 1.73) |
1.08 (0.58, 2.00) |
1.27 (0.22, 7.27) |
1.69 (0.74, 3.90) |
2-OS |
0.99 (0.47, 2.09) |
1.11 (0.36, 3.40) |
1.07 (0.41, 2.78) |
1.07 (0.28, 4.02) |
0.55 (0.18, 1.66) |
1.19 (0.37, 3.82) |
1.10 (0.38, 3.22) |
MACOP-B |
1.06 (0.58, 1.91) |
0.93 (0.57, 1.50) |
1.14 (0.60, 2.18) |
1.34 (0.23, 7.75) |
1.79 (0.76, 4.21) |
||
0.92 (0.46, 1.86) |
1.03 (0.35, 3.07) |
1.00 (0.40, 2.50) |
0.99 (0.27, 3.64) |
0.51 (0.18, 1.49) |
1.11 (0.36, 3.46) |
1.02 (0.36, 2.90) |
0.93 (0.33, 2.59) |
PACEBOM |
0.88 (0.46, 1.67) |
1.08 (0.60, 1.93) |
1.27 (0.22, 7.17) |
1.69 (0.75, 3.80) |
||
0.77 (0.35, 1.71) |
0.87 (0.27, 2.75) |
0.84 (0.31, 2.26) |
0.84 (0.22, 3.23) |
0.43 (0.14, 1.34) |
0.94 (0.28, 3.08) |
0.86 (0.29, 2.60) |
0.78 (0.38, 1.62) |
0.84 (0.29, 2.42) |
ProMACE-CytaBOM |
1.23 (0.61, 2.46) |
1.45 (0.25, 8.52) |
1.93 (0.79, 4.72) |
||
1.06 (0.52, 2.12) |
1.18 (0.40, 3.52) |
1.14 (0.46, 2.86) |
1.14 (0.31, 4.17) |
0.59 (0.20, 1.71) |
1.27 (0.41, 3.96) |
1.17 (0.41, 3.32) |
1.07 (0.38, 2.97) |
1.15 (0.43, 3.09) |
1.36 (0.47, 3.91) |
R-CHOP |
1.18 (0.23, 6.01) |
1.57 (0.67, 3.68) |
||
1.61 (0.11, 23.30) |
1.80 (0.11, 29.63) |
1.74 (0.11, 26.95) |
1.73 (0.10, 31.18) |
0.90 (0.05, 14.65) |
1.94 (0.12, 32.52) |
1.79 (0.11, 28.87) |
1.62 (0.10, 26.10) |
1.74 (0.11, 27.70) |
2.07 (0.13, 33.71) |
1.52 (0.12, 20.12) |
R-HDS |
1.33 (0.21, 8.39) |
||
1.27 (0.47, 3.46) |
1.42 (0.39, 5.25) |
1.38 (0.43, 4.41) |
1.37 (0.31, 6.05) |
0.71 (0.20, 2.57) |
1.54 (0.40, 5.87) |
1.41 (0.40, 5.00) |
1.29 (0.37, 4.48) |
1.38 (0.41, 4.69) |
1.64 (0.46, 5.88) |
1.21 (0.36, 4.09) |
0.79 (0.05, 13.78) |
VMP |
||
3-OS |
CHOP |
0.86 (0.61, 1.22) |
0.83 (0.66, 1.04) |
1.75 (1.15, 2.68) |
0.96 (0.67, 1.38) |
0.88 (0.63, 1.24) |
0.81 (0.53, 1.24) |
0.85 (0.62, 1.16) |
0.70 (0.40, 1.23) |
0.83 (0.62, 1.11) |
0.92 (0.25, 3.36) |
1.58 (0.81, 3.08) |
5-OS |
|
0.85 (0.59, 1.24) |
ACE |
0.96 (0.74, 1.25) |
2.03 (1.18, 3.52) |
1.11 (0.67, 1.84) |
1.02 (0.63, 1.67) |
0.94 (0.54, 1.63) |
0.99 (0.62, 1.57) |
0.82 (0.42, 1.58) |
0.97 (0.62, 1.51) |
1.06 (0.28, 4.08) |
1.83 (0.87, 3.89) |
|||
0.84 (0.66, 1.07) |
0.98 (0.75, 1.30) |
ACVBP |
2.12 (1.31, 3.43) |
1.16 (0.76, 1.79) |
1.07 (0.71, 1.61) |
0.98 (0.60, 1.59) |
1.03 (0.70, 1.51) |
0.85 (0.47, 1.56) |
1.01 (0.70, 1.45) |
1.11 (0.30, 4.15) |
1.91 (0.94, 3.87) |
|||
1.69 (1.06, 2.72) |
1.99 (1.09, 3.62) |
2.02 (1.18, 3.44) |
CNOP |
0.55 (0.31, 0.96) |
0.50 (0.29, 0.87) |
0.46 (0.25, 0.84) |
0.49 (0.29, 0.82) |
0.40 (0.20, 0.81) |
0.48 (0.28, 0.79) |
0.52 (0.13, 2.05) |
0.90 (0.41, 1.99) |
|||
0.81 (0.51, 1.31) |
0.95 (0.52, 1.74) |
0.97 (0.57, 1.65) |
0.48 (0.25, 0.94) |
I-CHOP |
0.92 (0.56, 1.52) |
0.84 (0.48, 1.48) |
0.89 (0.55, 1.43) |
0.73 (0.38, 1.43) |
0.87 (0.54, 1.38) |
0.95 (0.25, 3.68) |
1.65 (0.77, 3.52) |
|||
0.90 (0.62, 1.30) |
1.05 (0.62, 1.78) |
1.07 (0.68, 1.67) |
0.53 (0.29, 0.97) |
1.10 (0.60, 2.02) |
m-BACOD |
0.92 (0.53, 1.59) |
0.96 (0.61, 1.53) |
0.80 (0.42, 1.54) |
0.94 (0.60, 1.47) |
1.04 (0.27, 3.99) |
1.79 (0.85, 3.79) |
|||
0.78 (0.51, 1.17) |
0.91 (0.52, 1.58) |
0.92 (0.57, 1.49) |
0.46 (0.24, 0.86) |
0.95 (0.51, 1.79) |
0.86 (0.50, 1.51) |
MACOP-B |
1.05 (0.62, 1.78) |
0.87 (0.43, 1.75) |
1.03 (0.61, 1.72) |
1.13 (0.29, 4.44) |
1.95 (0.88, 4.31) |
|||
0.84 (0.60, 1.19) |
0.99 (0.60, 1.63) |
1.01 (0.66, 1.53) |
0.50 (0.28, 0.89) |
1.04 (0.58, 1.86) |
0.94 (0.57, 1.56) |
1.09 (0.64, 1.86) |
PACEBOM |
0.83 (0.44, 1.57) |
0.98 (0.64, 1.50) |
1.08 (0.28, 4.11) |
1.86 (0.89, 3.89) |
|||
0.78 (0.49, 1.25) |
0.92 (0.50, 1.67) |
0.93 (0.55, 1.58) |
0.46 (0.24, 0.90) |
0.96 (0.49, 1.88) |
0.87 (0.48, 1.59) |
1.01 (0.66, 1.55) |
0.93 (0.52, 1.65) |
ProMACE-CytaBOM |
1.18 (0.63, 2.21) |
1.30 (0.32, 5.35) |
2.24 (0.94, 5.36) |
|||
0.70 (0.51, 0.96) |
0.82 (0.51, 1.34) |
0.83 (0.56, 1.25) |
0.41 (0.23, 0.73) |
0.86 (0.49, 1.53) |
0.78 (0.48, 1.28) |
0.91 (0.54, 1.52) |
0.83 (0.52, 1.32) |
0.90 (0.51, 1.58) |
R-CHOP |
1.10 (0.31, 3.91) |
1.90 (0.92, 3.93) |
|||
0.69 (0.15, 3.13) |
0.80 (0.17, 3.83) |
0.82 (0.18, 3.80) |
0.41 (0.08, 1.98) |
0.85 (0.17, 4.14) |
0.77 (0.16, 3.65) |
0.89 (0.18, 4.26) |
0.81 (0.17, 3.84) |
0.88 (0.18, 4.29) |
0.98 (0.22, 4.31) |
R-HDS |
1.72 (0.40, 7.43) |
|||
1.54 (0.77, 3.09) |
1.80 (0.82, 3.97) |
1.83 (0.87, 3.84) |
0.91 (0.39, 2.11) |
1.89 (0.81, 4.40) |
1.71 (0.78, 3.78) |
1.98 (0.88, 4.46) |
1.82 (0.84, 3.95) |
1.96 (0.85, 4.56) |
2.19 (1.02, 4.72) |
2.24 (0.42, 11.87) |
VMP |
* Treatment, further description of each treatment can be seen in Supplementary Table 1.
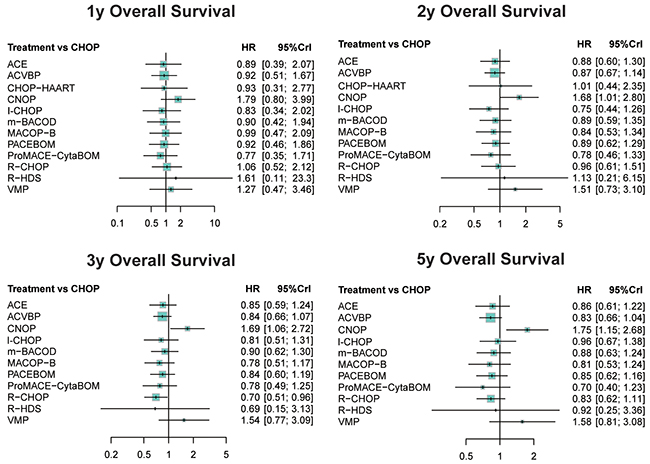
Figure 3: Forest plots for overall survival of non-Hodgkin lymphoma treatments.
CR results from NMA
The OR with 95% CrI was further evaluated to compare CR efficacy in Table 3. Patients treated with R-HDS exhibited significantly higher CR rate compared to both CNOP (OR=8.17; 95% CrIs=1.02-70.81) and VMP (OR=0.11; 95% CrIs=0.01-0.90), suggesting the better efficacy of R-HDS in respect of CR outcome. Forest plots for CR based on the comparison to CHOP were demonstrated in Figure 4, and no significant difference was presented.
Table 3: Complete remission of non-Hodgkin lymphoma treatments
CHOP |
0.54 (0.06, 5) |
1.07 (0.32, 3.63) |
2.03 (0.47, 8.58) |
0.51 (0.13, 1.88) |
1.17 (0.35, 4.06) |
1.25 (0.36, 4.31) |
0.94 (0.34, 2.69) |
1.58 (0.46, 5.26) |
0.89 (0.32, 2.64) |
1.13 (0.48, 2.89) |
4.18 (0.8, 21.98) |
0.44 (0.11, 1.73) |
0.92 (0.16, 5.16) |
ACE |
0.99 (0.29, 3.46) |
1.86 (0.2, 17.81) |
0.47 (0.05, 4.14) |
1.07 (0.13, 9.03) |
1.15 (0.14, 9.49) |
0.86 (0.12, 6.69) |
1.45 (0.17, 11.94) |
0.82 (0.11, 6.42) |
1.04 (0.16, 7.61) |
3.82 (0.36, 42.95) |
0.4 (0.04, 3.63) |
0.93 (0.28, 3.13) |
1.08 (0.19, 6.11) |
ACVBP |
1.88 (0.28, 12.43) |
0.47 (0.08, 2.8) |
1.08 (0.2, 6.23) |
1.16 (0.2, 6.55) |
0.87 (0.18, 4.44) |
1.46 (0.26, 8.08) |
0.83 (0.17, 4.26) |
1.05 (0.24, 4.95) |
3.86 (0.51, 30.88) |
0.41 (0.07, 2.48) |
0.49 (0.12, 2.12) |
2.14 (0.24, 19.11) |
0.53 (0.08, 3.53) |
CHOP-HARRT |
0.25 (0.03, 1.77) |
0.58 (0.09, 3.86) |
0.61 (0.09, 4.1) |
0.46 (0.08, 2.8) |
0.77 (0.12, 5.05) |
0.44 (0.08, 2.75) |
0.56 (0.1, 3.19) |
2.01 (0.23, 18.73) |
0.22 (0.03, 1.63) |
1.97 (0.53, 7.54) |
0.93 (0.11, 7.61) |
2.12 (0.36, 13.2) |
4.01 (0.57, 28.79) |
CNOP |
2.32 (0.39, 14.59) |
2.46 (0.4, 15.18) |
1.86 (0.35, 10.28) |
3.13 (0.52, 18.92) |
1.77 (0.33, 9.97) |
2.25 (0.47, 11.47) |
8.17 (1.02, 70.81) |
0.88 (0.13, 5.87) |
0.85 (0.25, 2.86) |
0.87 (0.11, 7.24) |
0.92 (0.16, 5.05) |
1.73 (0.26, 11.47) |
0.43 (0.07, 2.59) |
I-CHOP |
1.06 (0.19, 5.81) |
0.8 (0.16, 4.06) |
1.34 (0.23, 7.54) |
0.76 (0.15, 3.86) |
0.96 (0.22, 4.48) |
3.53 (0.46, 27.94) |
0.38 (0.06, 2.32) |
0.8 (0.23, 2.77) |
1.16 (0.15, 8.58) |
0.86 (0.15, 4.95) |
1.63 (0.24, 10.8) |
0.41 (0.07, 2.48) |
0.94 (0.17, 5.31) |
m-BACOD |
0.76 (0.15, 3.82) |
1.26 (0.22, 7.1) |
0.71 (0.14, 3.74) |
0.9 (0.2, 4.35) |
3.32 (0.43, 26.58) |
0.35 (0.06, 2.2) |
1.06 (0.37, 2.94) |
0.69 (0.08, 5.87) |
1.15 (0.23, 5.53) |
2.16 (0.36, 12.55) |
0.54 (0.1, 2.83) |
1.25 (0.25, 6.11) |
1.32 (0.26, 6.49) |
MACOP-B |
1.68 (0.32, 8.08) |
0.95 (0.34, 2.69) |
1.21 (0.31, 4.81) |
4.44 (0.62, 30.57) |
0.47 (0.08, 2.53) |
0.63 (0.19, 2.18) |
1.22 (0.16, 8.94) |
0.68 (0.12, 3.86) |
1.3 (0.2, 8.58) |
0.32 (0.05, 1.92) |
0.75 (0.13, 4.26) |
0.79 (0.14, 4.57) |
0.59 (0.12, 3.13) |
PACEBOM |
0.57 (0.12, 2.97) |
0.72 (0.17, 3.42) |
2.64 (0.35, 20.7) |
0.28 (0.05, 1.73) |
1.13 (0.38, 3.16) |
0.96 (0.13, 6.42) |
1.21 (0.23, 5.87) |
2.27 (0.36, 13.33) |
0.57 (0.1, 3.03) |
1.31 (0.26, 6.49) |
1.4 (0.27, 6.96) |
1.05 (0.37, 2.97) |
1.77 (0.34, 8.5) |
ProMACE-CytaBOM |
1.27 (0.32, 5.1) |
4.66 (0.65, 33.12) |
0.5 (0.09, 2.69) |
0.89 (0.35, 2.1) |
0.26 (0.02, 2.8) |
0.95 (0.2, 4.18) |
1.79 (0.31, 9.58) |
0.44 (0.09, 2.12) |
1.04 (0.22, 4.62) |
1.11 (0.23, 4.9) |
0.83 (0.21, 3.19) |
1.39 (0.29, 6.05) |
0.79 (0.2, 3.1) |
R-CHOP |
3.67 (0.9, 14.73) |
0.39 (0.08, 1.93) |
0.24 (0.05, 1.25) |
2.48 (0.28, 22.42) |
0.26 (0.03, 1.97) |
0.5 (0.05, 4.31) |
0.12 (0.01, 0.98) |
0.28 (0.04, 2.16) |
0.3 (0.04, 2.34) |
0.23 (0.03, 1.62) |
0.38 (0.05, 2.86) |
0.21 (0.03, 1.54) |
0.27 (0.07, 1.12) |
R-HDS |
0.11 (0.01, 0.9) |
2.27 (0.58, 8.85) |
2.48 (0.28, 22.42) |
2.44 (0.4, 15.18) |
4.62 (0.61, 33.45) |
1.14 (0.17, 7.69) |
2.66 (0.43, 16.95) |
2.83 (0.45, 17.64) |
2.14 (0.39, 12.06) |
3.56 (0.58, 21.76) |
2.01 (0.37, 11.7) |
2.59 (0.52, 13.33) |
9.39 (1.12, 81.45) |
VMP |
* Treatment, further description of each treatment can be seen in Supplementary Table 1.
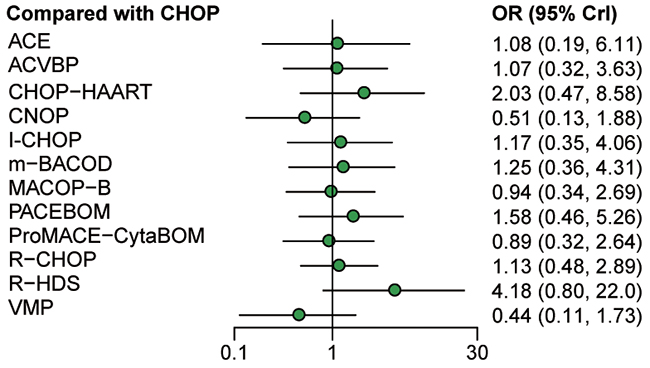
Figure 4: Forest plots for complete remission of non-Hodgkin lymphoma treatments.
SUCRA
For the purpose of estimating the ranking possibility of 13 treatments under each outcome, SUCRA values were calculated. As was shown in Table 4, both CNOP and VMP exhibited unsatisfying results with respect to all survival outcomes and CR. Therefore, CNOP and VMP regimens were not recommended based on the NMA results. Taking both short-term and long-term survival outcomes into account, ProMACE-CytaBOM seemed to be the most effective one since its SUCRA values under each survival outcome exceeded 0.6. In the meantime, R-CHOP had the potential to benefit long-term survival for its desirable performance in 3-year OS and 5-year OS while I-CHOP may significantly improve short-term survival outcomes for its relative high ranking in 1-year and 2-year OS. Moreover, the use of PACEBOM and CHOP-HARRT may also help control the development of NHL for their high ranking on CR.
Table 4: SUCRA value of non-Hodgkin lymphoma treatments
Treatment* |
1y-OS |
2y-OS |
3y-OS |
5y-OS |
CR |
|---|---|---|---|---|---|
ACE |
0.581 |
0.592 |
0.548 |
0.587 |
0.455 |
ACVBP |
0.563 |
0.613 |
0.575 |
0.664 |
0.451 |
CHOP |
0.494 |
0.407 |
0.309 |
0.344 |
0.396 |
CHOP-HARRT |
0.550 |
0.462 |
- |
- |
0.701 |
CNOP |
0.162 |
0.093 |
0.058 |
0.057 |
0.146 |
I-CHOP |
0.627 |
0.746 |
0.603 |
0.449 |
0.499 |
m-BACOD |
0.578 |
0.578 |
0.488 |
0.559 |
0.533 |
MACOP-B |
0.504 |
0.629 |
0.662 |
0.661 |
0.374 |
PACEBOM |
0.564 |
0.576 |
0.563 |
0.612 |
0.645 |
ProMACE-CytaBOM |
0.684 |
0.703 |
0.644 |
0.778 |
0.347 |
R-CHOP |
0.463 |
0.492 |
0.787 |
0.644 |
0.482 |
R-HDS |
0.369 |
0.434 |
0.640 |
0.521 |
0.854 |
VMP |
0.361 |
0.177 |
0.123 |
0.123 |
0.118 |
Higher SUCRA values represent better outcomes
Abbreviation: OS, overall survival; CR, complete remission
* Treatment, further description of each treatment can be seen in Supplementary Table 1
DISCUSSION
In this NMA, 13 different regimens of chemotherapies were compared in respect to therapeutic efficacy and prognosis outcomes in NHL patients. After direct evidence from 14 individual publications was extracted and both direct and indirect data was synthesized through network analysis, the statistical results regarding OS, CR and relative ranking could serve as supportive information to optimize the treatment strategy on the basis of individual disease condition.
As concluded in the results mentioned above, CNOP and VMP are recognized as the least effective regimens. Third-generation chemo regimens ProMACE-CytaBOM performed relatively better on OS outcomes, although its superiority did not maintain in CR. As for CR, R-HDS possessed a significantly remarkable efficacy, regardless of its modest performance in respect of OS. Additionally, R-CHOP, a standard treatment for DLBCL in International Prognostic Index, ranked top in 3 year- and 5 year-OS, which indicates its value in achieving greater long term prognosis among all types of NHL while I-CHOP was effective in short-term survival outcomes.
According to the results, there was little significant difference most of the treatments with respect to survival outcomes, however, their performance on CR differed from each other. Moreover, their performances on survival outcomes and CR were not consistent. R-HDS, ranked first in the SUCRA analysis with respect to CR, was compared with R-CHOP in Ladetto et.al, 2008 [18], and showed a significantly improved CR rate as well as event-free survival (EFS), while no significant difference detected in OS. As an advanced salvage second-line treatment which could ensure EFS in patients with relapse following R-CHOP, R-HDS might indicate its value in achieving superior disease control after first-line failure, but it is not an optimum choice at diagnosis because of its overtreatment as a front-line regimen.
Other than chemotherapy, NHL was also treated by well-established radiotherapy due to its sensitivity to radiation in early stages [28]. Previous radiation therapy techniques had been replaced by new ones based on modern integrating imaging, including intensity modulated radiation therapy and image guided radiation therapy which decreased the risk of normal tissue damage. Furthermore, their combination with chemotherapies consolidated chemotherapy’s response in local tumor control and provided an alternative option for patients suffering from chemo-resistant diseases or intolerant to chemotherapy without undermining the palliation of local symptoms [29]. Autologous stem cell transplantation was another way to improve survival for refractory aggressive NHL patients in the long term. However, it tended to relapse because of the reinfusion of the tumor cells in autologous graft. Adjuvant of rituximab administration to autologous transplantation is proved to have an impact to minimal residual disease to reduce relapse rate after transplantation in few studies [30-32].
We innovatively conducted the first NMA in NHL chemotherapeutic study. However, several limitations still existed in the NMA. Firstly, only 14 eligible studies were included corresponding to 13 different regimens, therefore, only data extracted from 1 or 2 studies were synthesized in view of each pair of comparators. Moreover, the published date of included studies ranged from 1992 to 2009. The most up-to-date data were absent from the NMA. Although several latest RCTs were conducted [9, 33], the lack of OS or CR outcomes for analysis leads to their exclusion from the NMA. The limited size of patients in this study and lack of head to head comparisons might undermine the credibility and authenticity of this assessment. Additional clinical trials were required to supplement further evaluation. Secondly, although adverse events were reported in some of the included studies, however, due to their absence in most of the studies, they were not included in this study. However, safety is also an important factor which is taken into serious consideration during clinical application. Some patients treated by MACOP-B experienced serious side effects including infections, mucositis and cardiac abnormities, and its application was somehow prevented despite its good performance on survival outcomes [20]. Therefore, the lack of safety analysis may weaken the clinical significance of this article, and more comprehensive studies should be done to offer more grounded conclusions.
In general, despite all the limitations, this was the very first NMA comparing different chemotherapeutics on their efficacy for patients with NHL, and the strict inclusion and exclusion criteria contributed to the reliability of this article.
To conclude, ProMACE-CytaBOM and R-HDS were recommended for their desirable performance on survival outcomes and CR, respectively. While R-CHOP and I-CHOP served as alternatives for the benefits they invited to long-term and short-term survival outcomes. However, more comprehensive studies with larger sample size and safety analysis were still needed.
MATERIALS AND METHODS
Search strategy and selection criteria
PubMed and Embase were used to perform literature searching by two reviewers to avoid bias. The key terms “non-Hodgkin lymphoma”, “randomized controlled trial” and different regimens described in Supplementary Table 1, such as “ACE”, “ACVBP”, “CHOP”, “CNOP”, etc. were included to formulate the searching query. In the identified literatures, duplications were removed and irrelevant records were excluded after abstract or full-text screening. The included studies were selected according to following criteria: (1) patients should be diagnosed with NHL; (2) studies should evaluate at least two of the analyzed treatments; (3) studies should be designed to be RCTs; (4) studies included prognosis and outcome parameters: OS and complete remission (CR). Eligible studies were included regardless of patient age, gender, conducting country or disease stage.
Data extraction
Data from eligible studies were extracted independently by two reviewers. The following data were extracted if available: (1) basic information, including authors, publication year, country, study size, follow-up duration; (2) baseline characteristics of patients including gender, age and disease stage; (3) treatment regimens; (4) primary efficacy outcomes, including short-term survival (1-year OS and 2-year OS), long-term survival (3-year OS and 5-year OS), and CR.
Statistical analysis
Both direct and indirect comparisons were conducted in Bayesian NMA using the STATA 13.0 and R 3.2.3 software and random-effect model was adopted to conduct the analysis. Hazard ratio (HR) were used to compare binary OS outcomes whereas odds ratio (OR) were calculated to evaluate CR between two different treatments in NMA, with their 95% credible intervals (CrIs) to evaluate the precision of corresponding statistics. Forest plots were used to visually present the relative therapeutic efficacy among different comparators. Moreover, surface under the cumulative ranking curve (SUCRA) of each treatment was measured in order to provide a hierarchy of treatments.
Abbreviations
non-Hodgkin lymphoma (NHL); increasing fractional dose of CHOP (I-CHOP); rituximab to CHOP (R-CHOP); randomized controlled trials (RCTs); network meta-analysis (NMA); complete remission (CR); Hazard ratio (HR); odds ratio (OR); credible intervals (CrIs).
Author contributions
Study design and conception: Pengcheng Cai; data collection and analysis: Jinjin Hao; manuscript drafting: Pengcheng Cai and Dan Wang; manuscript critical revision: Jiawei Xu; approving article publishing: all authors.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
FUNDING
None.
REFERENCES
1. Shankland KR, Armitage JO, Hancock BW. Non-Hodgkin lymphoma. Lancet. 2012; 380:848–57.
2. Campo E, Swerdlow SH, Harris NL, Pileri S, Stein H, Jaffe ES. The 2008 WHO classification of lymphoid neoplasms and beyond: evolving concepts and practical applications. Blood. 2011; 117:5019–32.
3. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015; 65:5–29.
4. Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015; 136:E359–86.
5. Lam CJ, Curtis RE, Dores GM, Engels EA, Caporaso NE, Polliack A, Warren JL, Young HA, Levine PH, Elmi AF, Fraumeni JF Jr, Tucker MA, Morton LM. Risk Factors for Melanoma Among Survivors of Non-Hodgkin Lymphoma. J Clin Oncol. 2015; 33:3096–104.
6. Martí-Carvajal AJ, Cardona AF, Lawrence A. Interventions for previously untreated patients with AIDS-associated non-Hodgkin’s lymphoma. Cochrane Database Syst Rev. 2009; CD005419.
7. Lyman GH, Crawford J, Tomita D, Whittaker S, Dale DC. Changing patterns of chemotherapy relative dose intensity and supportive care for aggressive B-cell non-Hodgkin lymphoma. Leuk Lymphoma. 2015.
8. Fisher RI, Gaynor ER, Dahlberg S, Oken MM, Grogan TM, Mize EM, Glick JH, Coltman CA Jr, Miller TP. Comparison of a standard regimen (CHOP) with three intensive chemotherapy regimens for advanced non-Hodgkin’s lymphoma. N Engl J Med. 1993; 328:1002–06.
9. Stopeck AT, Unger JM, Rimsza LM, LeBlanc M, Farnsworth B, Iannone M, Glenn MJ, Fisher RI, Miller TP. A phase 2 trial of standard-dose cyclophosphamide, doxorubicin, vincristine, prednisone (CHOP) and rituximab plus bevacizumab for patients with newly diagnosed diffuse large B-cell non-Hodgkin lymphoma: SWOG 0515. Blood. 2012; 120:1210–17.
10. Sehn LH, Berry B, Chhanabhai M, Fitzgerald C, Gill K, Hoskins P, Klasa R, Savage KJ, Shenkier T, Sutherland J, Gascoyne RD, Connors JM. The revised International Prognostic Index (R-IPI) is a better predictor of outcome than the standard IPI for patients with diffuse large B-cell lymphoma treated with R-CHOP. Blood. 2007; 109:1857–61.
11. Habermann TM, Weller EA, Morrison VA, Gascoyne RD, Cassileth PA, Cohn JB, Dakhil SR, Woda B, Fisher RI, Peterson BA, Horning SJ. Rituximab-CHOP versus CHOP alone or with maintenance rituximab in older patients with diffuse large B-cell lymphoma. J Clin Oncol. 2006; 24:3121–27.
12. Coiffier B, Lepage E, Briere J, Herbrecht R, Tilly H, Bouabdallah R, Morel P, Van Den Neste E, Salles G, Gaulard P, Reyes F, Lederlin P, Gisselbrecht C. CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N Engl J Med. 2002; 346:235–42.
13. Kaplan LD, Lee JY, Ambinder RF, Sparano JA, Cesarman E, Chadburn A, Levine AM, Scadden DT. Rituximab does not improve clinical outcome in a randomized phase 3 trial of CHOP with or without rituximab in patients with HIV-associated non-Hodgkin lymphoma: AIDS-Malignancies Consortium Trial 010. Blood. 2005; 106:1538–43.
14. Castillo JJ, Echenique IA. Rituximab in combination with chemotherapy versus chemotherapy alone in HIV-associated non-Hodgkin lymphoma: a pooled analysis of 15 prospective studies. Am J Hematol. 2012; 87:330–33.
15. Messori A, Vaiani M, Trippoli S, Rigacci L, Jerkeman M, Longo G. Survival in patients with intermediate or high grade non-Hodgkin’s lymphoma: meta-analysis of randomized studies comparing third generation regimens with CHOP. Br J Cancer. 2001; 84:303–07.
16. Gordon LI, Harrington D, Andersen J, Colgan J, Glick J, Neiman R, Mann R, Resnick GD, Barcos M, Gottlieb A, O’Connell M. Comparison of a second-generation combination chemotherapeutic regimen (m-BACOD) with a standard regimen (CHOP) for advanced diffuse non-Hodgkin’s lymphoma. N Engl J Med. 1992; 327:1342–49.
17. Haioun C, Mounier N, Emile JF, Ranta D, Coiffier B, Tilly H, Recher C, Ferme C, Gabarre J, Herbrecht R, Morchhauser F, Gisselbrecht C. Rituximab versus observation after high-dose consolidative first-line chemotherapy with autologous stem-cell transplantation in patients with poor-risk diffuse large B-cell lymphoma. Annals of oncology. 2009; 20:1985–1992.
18. Ladetto M, De Marco F, Benedetti F, Vitolo U, Patti C, Rambaldi A, Pulsoni A, Musso M, Liberati AM, Olivieri A, Gallamini A, Pogliani E, Rota Scalabrini D, et al, and Intergruppo Italiano Linfomi (IIL). Prospective, multicenter randomized GITMO/IIL trial comparing intensive (R-HDS) versus conventional (CHOP-R) chemoimmunotherapy in high-risk follicular lymphoma at diagnosis: the superior disease control of R-HDS does not translate into an overall survival advantage. Blood. 2008; 111:4004–13.
19. Linch DC, Smith P, Hancock BW, Hoskin PJ, Cunningham DC, Newland AC, Milligan D, Stevenson PA, Wood JK, Maclennan KA, Vaughan B, Vaughan G, Gregory WM. A randomized British National Lymphoma Investigation trial of CHOP vs. a weekly multi-agent regimen (PACEBOM) in patients with histologically aggressive non-Hodgkin’s lymphoma. Annals of oncology. 2000; 11:87–90.
20. Montserrat E, García-Conde J, Viñolas N, López-Guillermo A, Hernández-Nieto L, Zubizarreta A, Maldonado J, Alcalá A, Faura MV, Llorente A, Bladé J, Fontanillas M, Estapé J. CHOP vs. ProMACE-CytaBOM in the treatment of aggressive non-Hodgkin’s lymphomas: long-term results of a multicenter randomized trial.(PETHEMA: Spanish Cooperative Group for the Study of Hematological Malignancies Treatment, Spanish Society of Hematology). Eur J Haematol. 1996; 57:377–83.
21. Silingardi V, Federico M, Cavanna L, Avanzini P, Gobbi PG, Lombardo M, Carotenuto M, Frassoldati A, Pieresca C, Vallisa D, Merli F, Ascari E, Mauri C. ProMECE-CytaBOM vs MACOP-B in advanced aggressive non-Hodgkin’s lymphoma: long term results of a multicenter study of the Italian Lymphoma Study Group (GISL). Leuk Lymphoma. 1995; 17:313–20.
22. Sonneveld P, de Ridder M, van der Lelie H, Nieuwenhuis K, Schouten H, Mulder A, van Reijswoud I, Hop W, Lowenberg B. Comparison of doxorubicin and mitoxantrone in the treatment of elderly patients with advanced diffuse non-Hodgkin’s lymphoma using CHOP versus CNOP chemotherapy. J Clin Oncol. 1995; 13:2530–39.
23. Tilly H, Lepage E, Coiffier B, Blanc M, Herbrecht R, Bosly A, Attal M, Fillet G, Guettier C, Molina TJ, Gisselbrecht C, Reyes F, and Groupe d’Etude des Lymphomes de l’Adulte. Intensive conventional chemotherapy (ACVBP regimen) compared with standard CHOP for poor-prognosis aggressive non-Hodgkin lymphoma. Blood. 2003; 102:4284–89.
24. Tirelli U, Errante D, Van Glabbeke M, Teodorovic I, Kluin-Nelemans JC, Thomas J, Bron D, Rosti G, Somers R, Zagonel V, Noordijk EM. CHOP is the standard regimen in patients > or = 70 years of age with intermediate-grade and high-grade non-Hodgkin’s lymphoma: results of a randomized study of the European Organization for Research and Treatment of Cancer Lymphoma Cooperative Study Group. J Clin Oncol. 1998; 16:27–34.
25. Vaccher E, Spina M, di Gennaro G, Talamini R, Nasti G, Schioppa O, Vultaggio G, Tirelli U. Concomitant cyclophosphamide, doxorubicin, vincristine, and prednisone chemotherapy plus highly active antiretroviral therapy in patients with human immunodeficiency virus-related, non-Hodgkin lymphoma. Cancer. 2001; 91:155–63.
26. Verdonck LF, Notenboom A, de Jong DD, MacKenzie MA, Verhoef GE, Kramer MH, Ossenkoppele GJ, Doorduijn JK, Sonneveld P, van Imhoff GW. Intensified 12-week CHOP (I-CHOP) plus G-CSF compared with standard 24-week CHOP (CHOP-21) for patients with intermediate-risk aggressive non-Hodgkin lymphoma: a phase 3 trial of the Dutch-Belgian Hemato-Oncology Cooperative Group (HOVON). Blood. 2007; 109:2759–66.
27. Wolf M, Matthews JP, Stone J, Cooper IA, Robertson TI, Fox RM. Long-term survival advantage of MACOP-B over CHOP in intermediate-grade non-Hodgkin’s lymphoma. The Australian and New Zealand Lymphoma Group. Annals of oncology. 1997; 8:71–75.
28. Lowry L, Smith P, Qian W, Falk S, Benstead K, Illidge T, Linch D, Robinson M, Jack A, Hoskin P. Reduced dose radiotherapy for local control in non-Hodgkin lymphoma: a randomised phase III trial. Radiother Oncol. 2011; 100:86–92.
29. Illidge T, Specht L, Yahalom J, Aleman B, Berthelsen AK, Constine L, Dabaja B, Dharmarajan K, Ng A, Ricardi U, Wirth A, and International Lymphoma Radiation Oncology Group. Modern radiation therapy for nodal non-Hodgkin lymphoma-target definition and dose guidelines from the International Lymphoma Radiation Oncology Group. Int J Radiat Oncol Biol Phys. 2014; 89:49–58.
30. Horwitz SM, Negrin RS, Blume KG, Breslin S, Stuart MJ, Stockerl-Goldstein KE, Johnston LJ, Wong RM, Shizuru JA, Horning SJ. Rituximab as adjuvant to high-dose therapy and autologous hematopoietic cell transplantation for aggressive non-Hodgkin lymphoma. Blood. 2004; 103:777–83.
31. Papadaki T, Stamatopoulos K, Stavroyianni N, Paterakis G, Phisphis M, Stefanoudaki-Sofianatou K. Evidence for T-large granular lymphocyte-mediated neutropenia in Rituximab-treated lymphoma patients: report of two cases. Leuk Res. 2002; 26:597–600.
32. Press OW, Eary JF, Appelbaum FR, Martin PJ, Nelp WB, Glenn S, Fisher DR, Porter B, Matthews DC, Gooley T, et al. Phase II trial of 131I-B1 (anti-CD20) antibody therapy with autologous stem cell transplantation for relapsed B cell lymphomas. Lancet. 1995; 346:336–40.
33. Rummel MJ, Niederle N, Maschmeyer G, Banat GA, von Grünhagen U, Losem C, Kofahl-Krause D, Heil G, Welslau M, Balser C, Kaiser U, Weidmann E, Dürk H, et al, and Study group indolent Lymphomas (StiL). Bendamustine plus rituximab versus CHOP plus rituximab as first-line treatment for patients with indolent and mantle-cell lymphomas: an open-label, multicentre, randomised, phase 3 non-inferiority trial. Lancet. 2013; 381:1203–10.