
INTRODUCTION
Although surgical intervention after an early diagnosis is highly effective, the prognoses for metastatic renal cell carcinoma (MRCC), metastatic melanoma (MM), and pancreatic cancer (PC) remain poor. The median survival time of MRCC patients is 10 months [1], and the 5-year survival rate is less than 10% [2]. For MM patients, the median survival time is 8 to 9 months, and the 3-year survival rate is less than 15% [3]. PC patients have the lowest survival by stage of any solid tumor [4]. The development of new therapies, including VEGF axis inhibitors for MRCC and a BRAF inhibitor for MM, has helped improve survival rates in advanced patients. However, these drugs rarely induce a complete and enduring response. Checkpoint inhibitors, such as monoclonal antibodies against cytotoxic T-lymphocyte-associated antigen 4 and programmed death 1, represent a breakthrough in the treatment of solid tumors, including MRCC and MM [5, 6]. However, their high cost limits their clinical use, especially in developing countries.
At present, chemotherapy is still a common therapeutic approach for MRCC, MM and PC, although its efficacy is limited [7, 8]. For example, only 5% of advanced PC patients respond to treatment with gemcitabine and their median overall survival is only 5.7 months [9]. A clinical trial of combined gemcitabine/erlotinib treatment showed only a slight improvement, which increased median survival to 6.2 from the 5.9 months seen with gemcitabine alone [10]. In comparison to gemcitabine, FOLFIRINOX (oxaliplatin, irinotecan, fluorouracil, and leucovorin) or nab-paclitaxel plus gemcitabine therapy increased median overall survival by 4.3 and 1.8 months, respectively [11, 12]. However, these combined treatments are associated with a higher incidence of serious side effects, and patients must therefore undergo rigorous testing prior to chemotherapy and closer monitoring during treatment.
Since the discovery that interleukin-2 (IL-2) administration can benefit MM patients, the importance of tumor immunotherapy as a cancer treatment has grown [13, 14]. Rosenberg and colleagues found that adoptive cell transfer utilizing autologous tumor infiltrating lymphocytes helped 20 of 93 pretreated MM patients (22%) achieve a lasting complete response [15]. Implantation of cytokine-induced killer (CIK) cells has been a particularly promising adoptive immunotherapy, and their anti-tumor characteristics have proven clinically effective in treating many solid tumors [16–18]. In MRCC patients, adoptive transfer of CIK cells prolonged survival compared to combined IL-2 and interferon (IFN) α treatment [19]. However, additional research is needed to improve the efficacy of CIK cell treatments.
We previously found that CD11b+Gr-1+ myeloid-derived suppressor cells (MDSCs) inhibit anti-tumor immune responses and reduce the efficacy of immunotherapy in an animal model [20, 21]. In a clinical setting, low CD11b+CD33+HLA-DR− MDSC levels in peripheral blood were associated with improved prognosis in MRCC patients receiving CIK cell therapy [22]. Reducing MDSC levels delays tumor growth and prolongs survival [23, 24]. Recent studies demonstrate that conventional chemotherapeutic agents, such as gemcitabine and 5-fluorouracil, kill tumor-associated MDSCs [25, 26]. Tyrosine kinase inhibitors such as sunitinib also decrease MDSC levels in patients with renal cell carcinoma [27]. In addition, promoting differentiation of MDSCs into mature, non-suppressive cells using all-trans retinoic acid (ATRA) reduces MDSC levels in MRCC patients [28].
In this study, we retrospectively analyzed clinical data from 17 MRCC, 10 advanced PC and 26 MM patients to determine whether administration of chemotherapeutic agents enhanced the efficacy of CIK cell therapy. We also examined MDSC levels to determine whether they were decreased after chemotherapy drugs were used.
RESULTS
Patients
MRCC, PC, and MM patient characteristics are listed in Tables 1, 2 and 3, respectively. The groups were similar with respect to age, sex, and extent of disease. All patients had metastatic disease and Karnofsky performance status scores greater than 80.
MDSC levels before and after chemotherapy drug administration
Both 5-fluorouracil and gemcitabine prevent MDSC accumulation in tumor-bearing hosts [25, 26], while dacarbazine does not [29]. We confirmed these results by examining MDSC levels in the peripheral blood of cancer patients. Representative MDSC levels before and after chemotherapy are shown in Figure 1 for representative MRCC, MM, and PC patients.
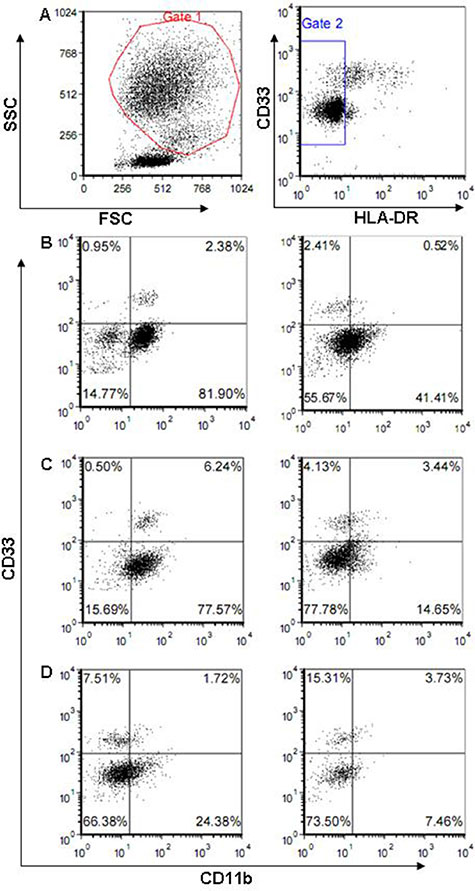
Figure 1: Flow cytometric analysis of peripheral blood mononuclear cells by FACScan. Data shown are for one representative MRCC (B), PC (C), and MM (D) patient before (left) and after (right) administration of 5-fluorouracil, gemcitabine, and dacarbazine, respectively. HLA-DR− cells detected in region 2 were divided into four fractions based on the expression of CD11b and CD33. CD11b+CD33+ cells were analyzed. Panel A shows the gate used to analyze MDSCs.
Survival and response
There were differences in survival between treatment groups in MRCC and PC patients. Kaplan-Meier curves for survival by treatment type are shown in Figure 2. One-year survival rates increased from 80% in MRCC patients receiving only CIK cell therapy to 100% in patients receiving both CIK cell treatment and chemotherapy (p = 0.035). At the completion of patient monitoring, 37% of CIK-treated MRCC patients were alive compared to 80% of patients receiving CIK cell treatment and chemotherapy (p = 0.035; Figure 2A). CIK-treated MRCC patients survived a median of 19.9 months (range: 3.7 to 33.1 months) after the first CIK cell infusion, while the median survival in patients receiving both CIK cell treatment and chemotherapy was 32.4 months (range: 21.3 to 41.9 months) (p = 0.0035; Figure 3A). Similarly, CIK-treated PC patients had lower 1-year survival rates (p = 0.002; Figure 2B) and median survival times (p = 0.001; Figure 3B) (0% and 5.6 months, range: 5.3 to 9.1) than PC patients treated with both CIK cells and chemotherapy (80% and 14.9 months, range: 12.0 to 22.1). However, there were no treatment-dependent differences in 1-year survival rate or median survival time (66.7% versus 71.4% (p = 0.92) and 13.9 versus 13.1 months (p = 0.39); Figures 2C and 3C) in MM patients.
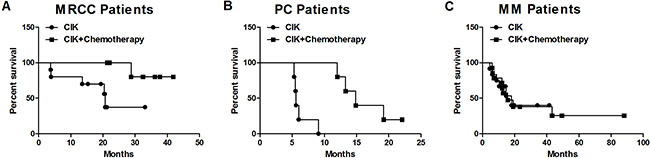
Figure 2: Survival curve for MRCC (A), PC (B), and MM (C) patients receiving CIK cell therapy alone and CIK cell therapy combined with chemotherapy.
Objective response rates did not differ depending on treatment in MRCC patients or MM patients. The disease control rate (DCR) was 70% in CIK-treated MRCC patients and 100% in CIK- and chemotherapy-treated patients (p = 0.23, Table 1 and Figure 4A). The DCRs following the same treatments in MM patients were 42% and 64%, respectively (p = 0.23, Table 3 and Figure 4C). In PC patients, however, DCRs were higher in those receiving CIK cells and chemotherapy than in those receiving only CIK cell treatment (100% and 20%, respectively, p = 0.048, Table 2 and Figure 4B).
Table 1: Characteristics of the MRCC patients
Patient No |
Age/Sex |
Historical type |
Metastases |
Therapy |
Outcome |
|---|---|---|---|---|---|
1 |
54/M |
Chromophobe |
Lung, bone |
Sunitinib + CIK |
PR, alive 32.4 months |
2 |
78/M |
Clear cell |
Lung, LN |
Chemotherapy + CIK |
SD, alive 21.3 months |
3 |
54/F |
Clear cell |
Liver |
Chemotherapy + CIK |
PR, alive 22.0 months |
4 |
63/F |
Clear cell |
Lung, bone |
Chemotherapy + CIK |
SD, alive 37.7 months |
5 |
71/M |
Clear cell |
Lung |
Chemotherapy + CIK |
SD, alive 36.1 months |
6 |
46/M |
Clear cell |
Lung |
Chemotherapy + CIK |
SD, alive 41.9 months |
7 |
64/F |
Clear cell |
Lung |
ATRA + CIK |
SD, died on month 28.8 |
8 |
65/M |
Clear cell |
Lung |
CIK |
PR, alive 19.4 months |
9 |
48/M |
Clear cell |
Brain, Lung, LN |
CIK |
PD, died on month 13.5 |
10 |
70/M |
Clear cell |
Lung, LN |
CIK |
SD, alive 15.3 months |
11 |
78/M |
Clear cell |
Lung |
CIK |
SD, died on month 20.4 |
12 |
72/M |
Clear cell |
Lung |
CIK |
SD, alive 21.2 months |
13 |
55/F |
Clear cell |
Lung, liver |
CIK |
SD, alive 33.1 months |
14 |
50/M |
Clear cell |
Liver, pancrea, LN |
CIK |
PD, died on month 3.9 |
15 |
21/F |
Clear cell |
Lung, liver, bone, LN |
CIK |
PD, died on month 3.7 |
16 |
54/M |
Papillary |
Lung |
CIK |
SD, alive 20.6 months |
17 |
49/M |
Clear cell |
Lung |
CIK |
SD, died on month 20.7 |
Abbreviations: LN, lymph nodes
Table 2: Characteristics of the PC patients
Patient No |
Age/Sex |
Diagnosed date |
Metastases |
Therapy |
Outcome |
|---|---|---|---|---|---|
1 |
70/M |
2010.09.01 |
Lung |
Chemotherapy + CIK |
SD, died on month 12.0 |
2 |
58/M |
2011.09.07 |
Abdominal LN |
Chemotherapy + CIK |
SD, died on month 13.3 |
3 |
49/F |
2011.09.07 |
Liver |
Chemotherapy + CIK |
SD, died on month 14.9 |
4 |
72/M |
2011.05.21 |
Liver |
Chemotherapy + CIK |
PR, died on month 19.2 |
5 |
52/M |
2011.06.1 |
Abdominal LN |
Chemotherapy + CIK |
SD, alive on 22.1 months |
6 |
75/F |
2010.10.16 |
Mesenterium |
CIK |
SD, died on month 9.1 |
7 |
66/M |
2012.04.20 |
Liver |
CIK |
PD, died on month 5.3 |
8 |
65/M |
2012.06.2 |
Bone, AC, PC |
CIK |
PD, died on month 5.5 |
9 |
43/F |
2012.07.1 |
Lung, Liver |
CIK |
PD, died on month 5.6 |
10 |
61/F |
2012.07.13 |
Liver |
CIK |
PD, died on month 6.0 |
Abbreviations: LN, lymph nodes; AC, abdominal cavity; PC, pelvic cavity
Table 3: Characteristics of the MM patients
Patient No |
Age/Sex |
Diagnosed date |
Metastases |
Therapy |
Outcome |
|---|---|---|---|---|---|
1 |
55/M |
2010.07.05 |
Lung, pleura, LN |
Chemotherapy + CIK |
PR, died on month 7.0 |
2 |
45/M |
2007.08.22 |
Lung, liver, bone |
Chemotherapy + CIK |
PD, died on month 43.3 |
3 |
37/F |
2012.04.13 |
Liver |
Chemotherapy + CIK |
SD, alive on 13.4 months |
4 |
48/F |
2010.04.10 |
Liver, LN |
Chemotherapy + CIK |
SD, died on month 19.0 |
5 |
53/M |
2011.09.21 |
Bone, LN |
Chemotherapy + CIK |
SD, died on month 6.2 |
6 |
47/F |
2006.01.15 |
Bone, Skin |
Chemotherapy + CIK |
CR, died on month 88.0 |
7 |
50/F |
2011.05.01 |
Lung, Spleen |
Chemotherapy + CIK |
PD, died on month 12.0 |
8 |
77/M |
2012.05.02 |
Lung |
Chemotherapy + CIK |
SD, alive on 12.8 months |
9 |
55/F |
2009.04.10 |
Lung, Liver |
Chemotherapy + CIK |
PD, alive on 49.3 months |
10 |
48/F |
2010.03.12 |
Lung, Bone, LN |
Chemotherapy + CIK |
SD, died on month 12.2 |
11 |
47/M |
2011.09.15 |
Lung, Liver, Bone, PC |
Chemotherapy + CIK |
PD, died on month 6.0 |
12 |
64/F |
2012.04.11 |
Lung, Liver, Skin |
Chemotherapy + CIK |
PR, died on month 12.8 |
13 |
26/M |
2011.06.09 |
Lung, Liver, Bone, Adrenaline |
Chemotherapy + CIK |
PD, died on month 15.6 |
14 |
38/M |
2011.06.23 |
LN |
Chemotherapy + CIK |
PR, alive on 23.1 months |
15 |
51/F |
2011.09.30 |
Brain, LN, Spleen |
CIK |
SD, alive on 19.8 months |
16 |
53/M |
2009.07.23 |
Lung, LN, PC |
CIK |
PD, Died on month 41.5 |
17 |
76/M |
2011.12.30 |
LN |
CIK |
PD, Died on month 4.5 |
18 |
55/F |
2010.07.26 |
Skin |
CIK |
SD, alive on 34.1 months |
19 |
76/F |
2012.04.12 |
LN |
CIK |
SD, alive on 13.4 months |
20 |
29/M |
2012.04.25 |
LN |
CIK |
SD, alive on 13.0 months |
21 |
44/F |
2011.05.24 |
Vagina, LN |
CIK |
PD, died on month 18.0 |
22 |
55/M |
2011.10.26 |
Liver, Stomach |
CIK |
PD, died on month 6.1 |
23 |
66/F |
2012.03.16 |
Lung, LN |
CIK |
SD, alive on 14.3 months |
24 |
48/F |
2011.04.14 |
Nasal cavity |
CIK |
PD, died on month 8.7 |
25 |
76/F |
2011.07.01 |
Skin, LN |
CIK |
PD, died on month 10.3 |
26 |
67/F |
2012.02.09 |
Lung, Skin |
CIK |
PD, died on month 14.5 |
Abbreviations: LN, lymph nodes; PC, pelvic cavity
Adverse effects
More severe treatment toxicity resulted from combined CIK cell treatment and chemotherapy than from CIK cell treatment alone. Specifically, combined treatment resulted in lower blood counts and increases in nonhematologic events, including nausea and vomiting, diarrhea, skin reactions, nerve changes, fatigue, and oral mucositis. The most common adverse effect of CIK cell therapy alone was fever, which occurred in approximately 15% patients. These patients recovered from this side effect either without treatment or after the oral administration of non-steroidal anti-inflammatory drugs such as indomethacin [22].
DISCUSSION
Our results suggest that combining chemotherapy with immunotherapy might improve survival in MRCC and PC patients. Recently, it was reported that combining gemcitabine and/or S-1 chemotherapy with dendritic cell vaccine immunotherapy prolongs median survival to 12 months [30], while the median survival was 8.8–10.1 months when these chemotherapy drugs were not combined with the immunotherapy (31). Here, we found that PC patients receiving CIK cell therapy combined with gemcitabine had a median survival time of 14.9 months as compared to 5.6 months in those receiving CIK cell treatment alone. In MRCC patients, combined CIK cell and chemotherapy treatment resulted in a 1-year survival rate of 100% as compared to 80% in those receiving only CIK cell therapy. MRCC patients receiving CIK cell treatment alone survived a median of 19.9 months, while those receiving CIK cell treatment and chemotherapy survived 32.4 months, suggesting that combining these therapies improves survival.
Furthermore, we found that decreased MDSC levels were associated with the superior efficacy of this combined therapy. CIK cells are mainly CD3+CD56+ cells, which express CD4 and CD8 and have natural killer (NK) cell activity [32–34]. The tumoricidal activity of CIK cells partly depends on their ability to produce IFNγ [35]. NKG2D-NKG2D ligand interactions, which are necessary for NK cell activation and cytolytic activity, also contribute to the antitumor activity of CIK cells [36]. It is thus possible that CIK cells exert antitumor effects by reducing the activity of immune inhibitory factors that target T and NK cells. MDSC levels increase dramatically during tumor progression, and MDSCs inhibit both T cells and NK cells in animal models and in cancer patients [37–39]. Therefore, depletion of MDSCs may represent a new approach to cancer immunotherapy. The commonly used chemotherapy drugs 5-fluorouracil, gemcitabine, sunitinib and ATRA all effectively decrease MDSC levels [25–28]. As expected, we show here that administration of these drugs to MRCC and PC patients receiving CIK cell immunotherapy prolonged survival time. Similar clinical observations in patients with other solid tumors have been reported recently. Combining chemotherapy (5-fluorouracil and oxaliplatin) with CIK cell treatment in patients with advanced gastric cancer improves quality of life and increases 2-year survival rate compared to treatment with chemotherapy alone [40]. Increased treatment efficacy has also been observed in advanced non-small cell lung cancer patients when docetaxel, which is also known to eliminate MDSCs, is combined with CIK cell therapy [41, 42].
Combining chemotherapy and immunotherapy may not improve outcomes for all types of cancer, however. Here, CIK-treated MM patients had similar median survival times with or without chemotherapy. This result may be due in part to the use of dacarbazine, a cytotoxic drug widely used for melanoma treatment, which does not affect T regulatory cells (Tregs), MDSC levels, or dendritic cell maturation [29]. It is possible that combining CIK cell therapy with a different MDSC-decreasing drug instead might improve survival in MM patients as well. A recent report found that chemotherapy-induced lymphodepletion is essential before cell transfer in MM patients because it eliminates immune inhibitory cells (e.g. Tregs or MDSCs) from the tumor microenvironment [43]. We are currently carrying out a clinical trial to evaluate the efficacy of combined docetaxel and CIK cell treatment in MM patients.
In addition to their direct cytotoxic effects on tumor cells, chemotherapy drugs likely improve survival by enhancing CIK cell immunotherapy. A recent study reported that gemcitabine and 5-fluorouracil do more than simply induce MDSC cell death. These two drugs appear to also activate the pro-apoptotic protein Bax (Bcl2-associated X protein) in MDSCs, which induces two separate molecular cascades. The first activates the production and release of pro-tumorigenic cytokines, eventually reducing anticancer immunity and promoting tumor growth. The second cascade induces MDSC apoptosis, thus enhancing the antitumor efficacy of these drugs [44]. Another recent report evaluated the effects of dacarbazine on antitumor immune responses. Although no change in MDSC levels was observed, dacarbazine triggered the upregulation of NKG2D ligands on tumor cells, leading to NK cell activation and IFNγ secretion. NK cell-derived IFNγ upregulates major histocompatibility complex class I molecules on tumor cells, rendering them sensitive to cytotoxic CD8+ T cells [29]. These examples of the immunogenic effects of chemotherapy drugs further suggest that combining them with immunotherapies can improve cancer prognoses.
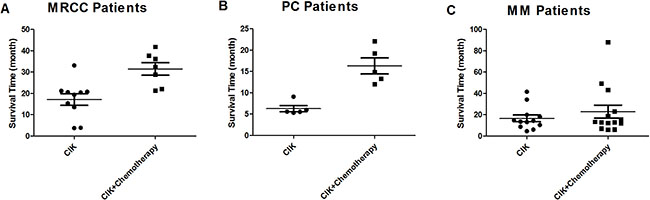
Figure 3: Median survival times for MRCC (A), PC (B), and MM (C) patients receiving CIK cell therapy alone and CIK cell therapy combined with chemotherapy.

Figure 4: Treatment response rates of MRCC (A), PC (B), and MM (C) patients receiving CIK cell therapy alone and CIK cell therapy combined with chemotherapy.
In contrast to murine models, a distinct and widely accepted marker combination for human MDSCs is still not available due to the heterogeneous nature of these immature cells, even within a single tumor type. For example, HLA-DR−Lin1low/−CD33+CD11b+ cells are designated MDSCs in patients with PC [45]. However, in another report, CD33+HLADR−CD11b+CD15+ cells and CD33+HLADR−/lowCD14+ cells were proposed as MDSCs, and both were elevated in PC [46]. Interestingly, recent research suggests that levels of two out of five antigens examined (HLA-DR and CD33, but not CD11b, CD14, or CD15) provide an accurate estimate of overall MDSC levels in PC [47]. Similarly, in MM patients, CD14+HLA-DRneg/low cells, CD14+IL4Ralpha+ cells, Lin−HLA-DR−CD33+ cells, CD15+IL4Ralpha+ cells, and CD14−CD66b+Arginase1+ cells were categorized as MDSCs [48–51]. We previously reported that, in MRCC patients, CD11b+CD33+HLA-DR– cells were MDSCs and their levels were correlated with patient outcome [22]. Thus, several populations of MDSCs have been identified, and it is likely that multiple populations are present in the peripheral blood mononuclear cells of patients with a single tumor type. In the present study, we defined MDSCs as CD11b+CD33+HLA− cells in MRCC, PC and MM. However, detailed investigation of specific MDSC subsets and their immunosuppressive activities in patients will help to improve cancer treatments.
Future studies should address two key limitations of the present experiments. First, the retrospective, non-randomized nature of this study, which included patients from only one hospital, may limit the generalizability of the results. Survival differences between patients receiving CIK cell treatment alone and in combination with chemotherapy might be affected by differences between groups during patient selection and differences in standard and supportive-care treatment. Second, the inclusion of a third patient group receiving only chemotherapy would have strengthened the results. However, the results of a previous retrospective analysis of 82 advanced PC patients suggest that combining CIK cell therapy with chemotherapy increased overall survival as compared to chemotherapy treatment alone. Together, these studies provide strong evidence that treatment efficacy increases when immunotherapy and chemotherapy are combined.
MATERIALS AND METHODS
Patients
Between March 19, 2010, and July 13, 2012, we enrolled 53 histologically-confirmed cancer patients from Henan Cancer Hospital & Affiliated Cancer Hospital of Zhengzhou University. 17 had MRCC with lung/liver metastases, 10 had advanced PC, and 26 had metastatic MM. All patients were separated into two cohorts. Patients in the first cohort received CIK cell therapy alone (CIK-treated); those in the second cohort received CIK cell therapy and chemotherapy. Eligible patients were at least 18 years of age and had a life expectancy of at least 12 weeks. All patients gave written informed consent, which was approved by the institutional review board of Zhengzhou University. This study was conducted in accordance with the provisions of the Declaration of Helsinki and Good Clinical Practice guidelines.
Treatment
Of the 17 MRCC patients, 10 patients were given CIK cell therapy alone and 7 were treated with CIK cell therapy combined with chemotherapy. The chemical agents used for the combined treatment included 2 cases of 5-fluorouracil (400 mg/m2, ivgtt, d1–5), 2 cases of gemcitabine (1000 mg/m2, ivgtt, d1, 8), 1 case of 5-fluorouracil plus gemcitabine, 1 case of sunitinib (50 mg, po, d1–28), and 1 case of ATRA (45 mg/m2, po, d1–28). Patients were given 1 cycle of 5-fluorouracil and/or gemcitabine every 3 weeks. After they completed all chemotherapy cycles (usually 2–6 cycles), these patients began to receive CIK cell therapy. For cases treated with oral sunitinib and ATRA, CIK cells were transfused concomitantly with chemotherapy drugs.
Of the 10 PC patients, 5 patients were given CIK cell therapy alone and 5 were given CIK cell therapy combined with gemcitabine-based chemotherapy (1000 mg/m2, ivgtt, d1, 8). Of the patients receiving combined treatment, 3 cases received CIK cell therapy after completing 2–6 cycles of chemotherapy (sequential combination treatment). The other 2 patients were given cycles of chemotherapy followed 2 days later by CIK cell transfusion (concomitant combination treatment); this treatment cycle was repeated 6 times.
Of the 26 MM patients, 12 were given CIK cell therapy alone and 14 were given CIK cell therapy combined with dacarbazine-based chemotherapy (300 mg/m2, ivgtt, d1–5). Of the patients receiving combined treatment, 5 received 2–6 cycles of sequential combination treatment, and the rest received 2–6 cycles of concomitant combination treatment.
CIK cell suspensions were prepared as described previously [22]. Briefly, peripheral blood mononuclear cells were separated and cultured under sterile conditions in 1640 medium containing anti-CD3 monoclonal antibody, IFNγ, IL-2, and RetroNectin (RN, Takara, Japan). After culturing the cells for 10 to 14 days, a target dose of about 5×109 CIK cells with over 95% viability was obtained and tested for biological contaminants. Cells were then prepared in sodium chloride solution containing 2% albumin before transfusion. After transfusion, patients were given IL-2 (two million IU per day) for 3 days to promote CIK cell activity. Patients in this study received at least 2 cycles of CIK cell transfusions.
For analysis of MDSCs, peripheral blood cells from MRCC, PC, and MM patients were collected aseptically by venipuncture, treated with BD FACS Lysing solution to lyse erythrocytes, stained with anti-CD33, anti-CD11b, and anti-HLA-DR monoclonal antibodies, and analyzed by flow cytometry. Peripheral blood was collected from each patient on 2 occasions. The first collection was done before chemotherapy and the second was done 15 days after chemotherapy was administered.
Evaluation of short-term efficacy and toxicity
Tumor response was separated into four categories according to the Response Evaluation Criteria in Solid Tumors (RECIST): complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD). CR, PR, and SD were included in the disease control rate (DCR). Tumors were assessed using computed tomographic (CT) scanning at baseline and 2 months after the initiation of treatment. Safety was assessed by examining records of adverse events. Hematologic and serum chemical measurements were performed before and after each cycle of treatment. Adverse events were graded using the Common Terminology Criteria for Adverse Events of the National Cancer Institute, version 3.0.
Statistical analysis
The statistical probability of survival was calculated according to the method of Kaplan and Meier. Differences between outcomes were compared using Log-rank (Mantel-Cox) Test. MDSC levels and survival times were compared between groups using unpaired t-tests. Fisher’s exact t-test was used to compare short-term efficacy between groups.
ACKNOWLEDGMENTS
The authors thank all of the patients who participated in this study and their families. The authors thank Dr. Torsten Juelich for linguistic assistance during the preparation of this manuscript.
GRANT SUPPORT
This work was supported by National Natural Science Foundation of China (81000914) and Foundation of He’nan Health Committee (2011010011).
CONFLICTS OF INTEREST
There is no conflicts of interest.
REFERENCES
1. Motzer RJ, Mazumdar M, Bacik J, Berg W, Amsterdam A, Ferrara J. Survival and prognostic stratification of 670 patients with advanced renal cell carcinoma. J Clin Oncol. 1999; 17:2530–2540.
2. Motzer RJ, Bander NH, Nanus DM. Renal-cell carcinoma. N Engl J Med. 1996; 335:865–875.
3. Balch CM, Gershenwald JE, Soong SJ, Thompson JF, Atkins MB, Byrd DR, Buzaid AC, Cochran AJ, Coit DG, Ding S, Eggermont AM, Flaherty KT, Gimotty PA, et al. Final version of 2009 AJCC melanoma staging and classification. J Clin Oncol. 2009; 27:6199–6206.
4. Siegel RL, Jemal A, Ward EM. Increase in incidence of colorectal cancer among young men and women in the United States. Cancer Epidemiol Biomarkers Prev. 2009; 18:1695–1698.
5. Harshman LC, Drake CG, Choueiri TK. PD-1 blockade in renal cell carcinoma: to equilibrium and beyond. Cancer Immunol Res. 2014; 2:1132–1141.
6. Luke JJ, Ott PA. PD-1 pathway inhibitors: the next generation of immunotherapy for advanced melanoma. Oncotarget. 2015; 28:3479–3492. doi:10.18632/oncotarget.2980.
7. Motzer RJ, Russo P. Systemic therapy for renal cell carcinoma. J Urol. 2000; 163:408–417.
8. Middleton MR, Grob JJ, Aaronson N, Fierlbeck G, Tilgen W, Seiter S, Gore M, Aamdal S, Cebon J, Coates A, Dreno B, Henz M, Schadendorf D, et al. Randomized phase III study of temozolomide versus dacarbazine in the treatment of patients with advanced metastatic malignant melanoma. J Clin Oncol. 2000; 18:158–166.
9. Burris HA 3rd, Moore MJ, Andersen J, Green MR, Rothenberg ML, Modiano MR, Cripps MC, Portenoy RK, Storniolo AM, Tarassoff P, Nelson R, Dorr FA, Stephens CD, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol. 1997; 15:2403–2413.
10. Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, Au HJ, Murawa P, Walde D, Wolff RA, Campos D, Lim R, Ding K, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol. 2007; 25:1960–1966.
11. Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, Adenis A, Raoul JL, Gourgou-Bourgade S, de la Fouchardière C, Bennouna J, Bachet JB, Khemissa-Akouz F, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011; 364:1817–1825.
12. Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, Seay T, Tjulandin SA, Ma WW, Saleh MN, Harris M, Reni M, Dowden S, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013; 369:1691–1703.
13. Rosenberg SA, Lotze MT, Muul LM, Leitman S, Chang AE, Ettinghausen SE, Matory YL, Skibber JM, Shiloni E, Vetto JT, Claudia AS, Colleen S, Cheryl MR. Observations on the systemic administration of autologous lymphokine-activated killer cells and recombinant interleukin-2 to patients with metastatic cancer. N Engl J Med. 1985; 313:1485–1492.
14. DeVita VT, Rosenberg SA. Two hundred years of cancer research. N Engl J Med. 2012; 366:2207–2214.
15. Rosenberg SA, Yang JC, Sherry RM, Kammula US, Hughes MS, Phan GQ, Citrin DE, Restifo NP, Robbins PF, Wunderlich JR, Morton KE, Laurencot CM, Steinberg SM, et al. Durable complete responses in heavily pretreated patients with metastatic melanoma using T-cell transfer immunotherapy. Clin Cancer Res. 2011; 17:4550–4557.
16. Thanendrarajan S, Kim Y, Schmidt-Wolf I. New adoptive immunotherapy strategies for solid tumours with CIK cells. Expert Opin Biol Ther. 2012; 12:565–572.
17. Sangiolo D. Cytokine induced killer cells as promising immunotherapy for solid tumors. J Cancer. 2011; 2:363–368.
18. Schmeel L, Schmeel F, Coch C, Schmidt-Wolf IG. Cytokine-induced killer (CIK) cells in cancer immunotherapy: report of the international registry on CIK cells (IRCC). J Cancer Res Clin Oncol. 2015; 141:839–849.
19. Liu L, Zhang W, Qi X, Li H, Yu J, Wei S, Hao X, Ren X. Randomized study of autologous cytokine-induced killer cell immunotherapy in metastatic renal carcinoma. Clin Cancer Res. 2012; 18:1751–1759.
20. Wang Z, Jiang J, Li Z, Zhang J, Wang H, Qin Z. A myeloid cell population induced by Freund adjuvant suppresses T-cell-mediated antitumor immunity. J Immunother. 2010; 33:167–177.
21. Jiang J, Wang Z, Li Z, Zhang J, Wang C, Xu X, Qin Z. Early exposure of high-dose interleukin-4 to tumor stroma reverses myeloid cell-mediated T-cell suppression. Gene Ther. 2101; 17:991–999.
22. Wang Z, Zhang Y, Liu Y, Wang L, Zhao L, Yang T, He C, Song Y, Gao Q. Association of myeloid-derived suppressor cells and efficacy of cytokine-induced killer cell immunotherapy in metastatic renal cell carcinoma patients. J Immunother. 2014; 37:43–50.
23. Filipazzi P, Huber V, Rivoltini L. Phenotype, function and clinical implications of myeloid-derived suppressor cells in cancer patients. Cancer Immunol Immunother. 2012; 61:255–263.
24. Montero AJ, Diaz-Montero CM, Kyriakopoulos CE, Bronte V, Mandruzzato S. Myeloid-derived suppressor cells in cancer patients: a clinical perspective. J Immunother. 2012; 35:107–115.
25. Suzuki E, Kapoor V, Jassar AS, Kaiser LR, Albelda SM. Gemcitabine selectively eliminates splenic Gr-1+/CD11b+ myeloid suppressor cells in tumor-bearing animals and enhances antitumor immune activity. Clin Cancer Res. 2005; 11:6713–6721.
26. Vincent J, Mignot G, Chalmin F, Ladoire S, Bruchard M, Chevriaux A, Martin F, Apetoh L, Rebe C, Ghiringhelli F. 5-Fluorouracil selectively kills tumor-associated myeloid-derived suppressor cells resulting in enhanced T cell-dependent antitumor immunity. Cancer Res. 2010; 70:3052–3061.
27. Ko JS, Zea AH, Rini BI, Ireland JL, Elson P, Cohen P, Golshayan A, Rayman PA, Wood L, Garcia J, Dreicer R, Bukowski R, Finke JH. Sunitinib mediates reversal of myeloid-derived suppressor cell accumulation in renal cell carcinoma patients. Clin Cancer Res. 2009; 15:2148–2157.
28. Mirza N, Fishman M, Fricke I, Dunn M, Neuger AM, Frost TJ, Lush RM, Antonia S, Gabrilovich DI. All-trans-retinoic acid improves differentiation of myeloid cells and immune response in cancer patients. Cancer Res. 2006; 66:9299–9307.
29. Hervieu A, Rebe C, Vegran F, Chalmin F, Bruchard M, Vabres P, Apetoh L, Ghiringhelli F, Mignot G. Dacarbazine-mediated upregulation of NKG2D ligands on tumor cells activates NK and CD8 T cells and restrains melanoma growth. J Invest Dermatol. 2013; 133:499–508.
30. Kimura Y, Tsukada J, Tomoda T, Takahashi H, Imai K, Shimamura K, Sunamura M, Yonemitsu Y, Shimodaira S, Koido S, Homma S, Okamoto M. Clinical and immunologic evaluation of dendritic cell-based immunotherapy in combination with gemcitabine and/or S-1 in patients with advanced pancreatic carcinoma. Pancreas. 2012; 41:195–205.
31. Ueno H, Ioka T, Ikeda M, Ohkawa S, Yanagimoto H, Boku N, Fukutomi A, Sugimori K, Baba H, Yamao K, Shimamura T, Sho M, Kitano M, et al. Randomized phase III study of gemcitabine plus S-1, S-1 alone, or gemcitabine alone in patients with locally advanced and metastatic pancreatic cancer in Japan and Taiwan: GEST study. J Clin Oncol. 2013; 31:1640–1648.
32. Schmidt-Wolf IG, Negrin RS, Kiem HP, Blume KG, Weissman IL. Use of a SCID mouse/human lymphoma model to evaluate cytokine-induced killer cells with potent antitumor cell activity. J Exp Med. 1991; 174:139–149.
33. Lu PH, Negrin RS. A novel population of expanded human CD3+CD56+ cells derived from T cells with potent in vivo antitumor activity in mice with severe combined immunodeficiency. J Immunol. 1994; 153:1687–1696.
34. Linn YC, Hui KM. Cytokine-induced killer cells: NK-like T cells with cytotolytic specificity against leukemia. Leuk Lymphoma. 2003; 44:1457–1462.
35. Verneris MR, Baker J, Edinger M, Negrin RS. Studies of ex vivo activated and expanded CD8+ NK-T cells in humans and mice. J Clin Immunol. 2002; 22:131–136.
36. Verneris MR, Karami M, Baker J, Jayaswal A, Negrin RS. Role of NKG2D signaling in the cytotoxicity of activated and expanded CD8+ T cells. Blood. 2004; 103:3065–3072.
37. Gabrilovich DI, Nagaraj S. Myeloid-derived suppressor cells as regulators of the immune system. Nat Rev Immunol. 2009; 9:162–174.
38. Brandau S, Trellakis S, Bruderek K, Schmaltz D, Steller G, Elian M, Suttmann H, Schenck M, Welling J, Zabel P, Lang S. Myeloid-derived suppressor cells in the peripheral blood of cancer patients contain a subset of immature neutrophils with impaired migratory properties. J Leukoc Biol. 2011; 89:311–317.
39. Hoechst B, Voigtlaender T, Ormandy L, Gamrekelashvili J, Zhao F, Wedemeyer H, Lehner F, Manns MP, Greten TF, Korangy F. Myeloid derived suppressor cells inhibit natural killer cells in patients with hepatocellular carcinoma via the NKp30 receptor. Hepatology. 2009; 50:799–807.
40. Jiang J, Xu N, Wu C, Deng H, Lu M, Li M, Xu B, Wu J, Wang R, Xu J, Nilsson-Ehle P. Treatment of advanced gastric cancer by chemotherapy combined with autologous cytokine-induced killer cells. Anticancer Res. 2006; 26:2237–2242.
41. Kodumudi KN, Woan K, Gilvary DL, Sahakian E, Wei S, Djeu JY. A novel chemoimmunomodulating property of docetaxel: suppression of myeloid-derived suppressor cells in tumor bearers. Clin Cancer Res. 2010; 16:4583–4594.
42. Wu C, Jiang J, Shi L, Xu N. Prospective study of chemotherapy in combination with cytokine-induced killer cells in patients suffering from advanced non-small cell lung cancer. Anticancer Res. 2008; 28:3997–4002.
43. Dudley ME, Wunderlich JR, Yang JC, Sherry RM, Topalian SL, Restifo NP, Royal RE, Kammula U, White DE, Mavroukakis SA, Rogers LJ, Gracia GJ, Jones SA, et al. Adoptive cell transfer therapy following non-myeloablative but lymphodepleting chemotherapy for the treatment of patients with refractory metastatic melanoma. J Clin Oncol. 2005; 23:2346–2357.
44. Bruchard M, Mignot G, Derangère V, Chalmin F, Chevriaux A, Végran F, Boireau W, Simon B, Ryffel B, Connat JL, Kanellopoulos J, Martin F, Rébé C, et al. Chemotherapy-triggered cathepsin B release in myeloid-derived suppressor cells activates the Nlrp3 inflammasome and promotes tumor growth. Nat Med. 2013; 19:57–64.
45. Gabitass RF, Annels NE, Stocken DD, Pandha HA, Middleton GW. Elevated myeloid-derived suppressor cells in pancreatic, esophageal and gastric cancer are an independent prognostic factor and are associated with significant elevation of the Th2 cytokine interleukin-13. Cancer Immunol Immunother. 2011; 60:1419–1430.
46. Mundy-Bosse BL, Young GS, Bauer T, Binkley E, Bloomston M, Bill MA, Bekaii-Saab T, Carson WE 3rd, Lesinski GB. Distinct myeloid suppressor cell subsets correlate with plasma IL-6 and IL-10 and reduced interferon-alpha signaling in CD4+ T cells from patients with GI malignancy. Cancer Immunol Immunother. 2011; 60:1269–1279.
47. Markowitz J, Brooks TR, Duggan MC, Paul BK, Pan X, Wei L, Abrams Z, Luedke E, Lesinski GB, Mundy-Bosse B, Bekaii-Saab T, Carson WE 3rd. Patients with pancreatic adenocarcinoma exhibit elevated levels of myeloid-derived suppressor cells upon progression of disease. Cancer Immunol Immunother. 2015; 64:149–159.
48. Poschke I, Mougiakakos D, Hansson J, Masucci GV, Kiessling R. Immature immunosuppressive CD14+HLA-DR-/low cells in melanoma patients are Stat3hi and overexpress CD80, CD83, and DC-sign. Cancer Res. 2010; 70:4335–4345.
49. Filipazzi P, Valenti R, Huber V, Pilla L, Canese P, Iero M, Castelli C, Mariani L, Parmiani G, Rivoltini L. Identification of a new subset of myeloid suppressor cells in peripheral blood of melanoma patients with modulation by a granulocyte-macrophage colony-stimulation factor-based antitumor vaccine. J Clin Oncol. 2007; 25:2546–2553.
50. Mandruzzato S, Solito S, Falisi E, Francescato S, Chiarion-Sileni V, Mocellin S, Zanon A, Rossi CR, Nitti D, Bronte V, Zanovello P. IL4Ralpha+ myeloid-derived suppressor cell expansion in cancer patients. J Immunol. 2009; 182:6562–6568.
51. Schilling B, Sucker A, Griewank K, Zhao F, Weide B, Görgens A, Giebel B, Schadendorf D, Paschen A. Vemurafenib reverses immunosuppression by myeloid derived suppressor cells. Int J Cancer. 2013; 133:1653–1663.