
INTRODUCTION
Chinese patent medicines (CPMs), as a new fashion to modernize traditional Chinese medicine (TCM), play an increasingly important role in China's medical practice. CPMs are produced by modern manufacturing processes in forms such as capsules and injections [1]. CPMs, together with Western medicines (WMs) and Chinese herbal medicines, are the three categories of drugs in China's National Basic Medical Insurance Drug Catalogue (NBMIDC) [2], since China launched the National Basic Medical Insurance System in 1998. Anticancer CPMs is a special category in NBMIDC anticancer drugs. Recently, several hospitals reported that anticancer CPMs are increasingly being used in cancer treatment, and even growing faster than Western drugs [3–5]. Moreover, TCM has showed bright prospects not only in the discovery of anticancer drugs [6], but also in the systematic therapy for complex diseases [7]. With the wide use and increasing interest of CPMs in cancer treatment, a comprehensive and in-depth analysis for anticancer CPMs is urgently required.
To meet such urgent needs, we analyzed the data from the first nationwide survey into inpatients' utilization of health services covered by China's Urban Basic Medical Insurance from 2008 to 2010. This investigation was conducted by the China Health Insurance Research Association affiliated with the Ministry of Human Resources and Social Security of China. The health insurance data can provide rich information to describe the clinical care and drug use in a large scale [8, 9]. Based on 51,382 insured cancer inpatients from the nationwide survey, we for the first time revealed the use characteristics as well as herb-drug combined use patterns in China, offering valuable information to improve the rational use of anticancer drugs in the future.
RESULTS
Overall use of anticancer CPMs and WMs in sampled cancer patients
Of the 51,382 hospitalized cancer patients (Table S1), 67.9% (cost ratio 13.4%) used CPMs, 42.4% (cost ratio 9.1%; 2069 RMB cost per patient) used anticancer CPMs; 98.2% (cost ratio 86.4%) used WMs, and 51.7% (cost ratio 18.6%; 3458 RMB cost per patient) used anticancer WMs (Fig. 1A and 1B). Overall, 44,447 patients (87%) experienced 17 malignant cancers with each cancer having more than 500 cases (Table S2). 9 of the top 10 cancers are the same as those from a previously China national survey [10]. In top 17 cancers, use of 33 anticancer CPMs was highest in lung and nasopharynx cancer patients (both were 52%), and was higher than those using anticancer WMs (44% and 45%). Anticancer CPMs were also more commonly used than anticancer WMs for liver cancer (20% more), kidney cancer (14% more), pancreatic cancer (10% more), and esophagus cancer (8% more). By contrast, anticancer CPMs were used least for bladder cancer and leukemia of unspecified cell type (both were 21%) (Fig. 1C and 1D).
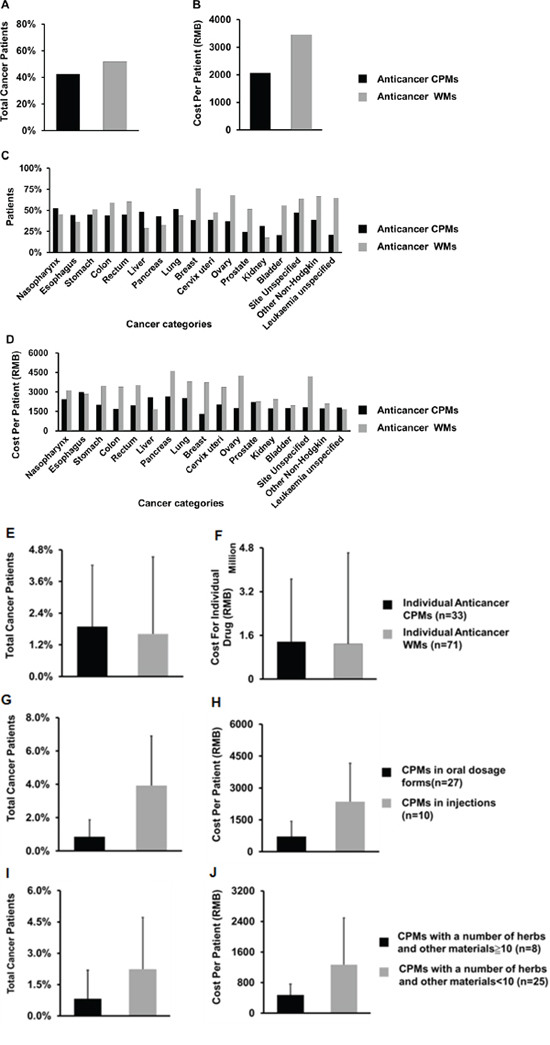
Figure 1. The overall use rate (A) and cost per patient (B) of 33 anticancer CPMs and 71 anticancer WMs, and their use rate (C) and cost per patient (D) in the top 17 cancers with a case number over 500. Use rate (E) and cost (F) of individual anticancer drugs in sampled cancer patients; use rate (G) and cost per patient (H) of anticancer CPMs in different formulations; use rate (I) and cost per patient (J) of anticancer CPMs with different numbers of raw materials.
Use of individual anticancer CPMs in sampled cancer patients
As shown in Fig. 1E–1J, the use rate (mean 1.9%) of individual anticancer CPMs in 51,382 cancer patients was significantly higher than that of individual anticancer WMs (mean 1.6%) (P = 0.017). There was no significant difference in the cost between individual anticancer CPMs (mean, 1.37 million RMB per drug) and that of individual anticancer WMs (mean, 1.29 million RMB per drug) (P = 0.069). Moreover, in subtypes of the anticancer CPMs, the use rate and cost of the CPMs injections or CPMs with less than 10 raw materials were significantly higher than those of oral formulations, or those with over 10 raw materials, respectively (all P < 0.05). The number of raw materials contained in an anticancer CPM was found to be significantly and negatively correlated with its usage (correlation coefficient = −0.449, P = 0.009; see data and diagram in Table S3).
Raw materials and efficacy of commonly used anticancer CPMs
By calculating the total use frequency of 33 anticancer CPMs with the same materials, the 10 mostly used raw materials are Huang-Qi (Astragali Radix), Ren-Shen (Ginseng Radix Et Rhizoma), Ku-Shen (Sophorae Flavescentis Radix), Ban-Mao (Mylabris), Ci-Wu-Jia (Acanthopanacis Senticosi Radix Et Rhizoma Seu Caulis), Dang-Shen (Codonopsis Pilosula), Nv-Zhen-Zi (Ligustri Lucidi Fructus), Tu-Fu-Ling (Smilacis Glabrae Rhizoma), Ban-Zhi-Lian (Scutellariae Barbatae Herba), and Ya-Dan-Zi (Bruceae Fructus). The therapy effects of anticancer CPMs are mainly expressed as two types of traditional efficacy in their instructions. One is “eliminating pathogen” (Qu-Xie in Chinese) labeled as clearing away hot, relieving blood stasis, removing toxin, etc. for those Antitumor CPMs. For instance, all top 3 antitumor CPMs have an efficacy of clearing away hot. The other is “strengthening body resistance” (Fu-Zheng in Chinese) labeled as tonifying Qi, nourishing yin, etc. for those Adjuvant antitumor CPMs. Table 1 listed the individual efficacy of top 15 anticancer CPMs with use frequency more than 500 patients.
Table 1: Raw materials, labeled efficacy, and use frequency of top 15 anticancer CPMs used in cancer patients (>500 cases)
CPM name |
NBMIDC subcategory |
Raw material |
Labeled efficacy |
Use frequency |
|---|---|---|---|---|
Shenqifuzheng Injection |
Adjuvant antitumor CPM |
Astragali Radix, Codonopsis Pilosula |
Tonifying Qi and strengthening body resistance |
4114 |
Fufangkushen Injection |
Antitumor CPM |
Sophorae Flavescentis Radix, Smilacis Glabrae Rhizoma |
Clearing away hot, removing dampness, cooling blood, removing toxin, resolving hard mass, and relieving pain |
3931 |
Aidi Injection |
Antitumor CPM |
Mylabris*, Ginseng Radix Et Rhizoma, Astragali Radix, Acanthopanacis Senticosi Radix Et Rhizoma Seu Caulis |
Clearing away hot, removing toxin, resolving stagnation and dispersing masses |
3761 |
Yadanziyou Injection (Oral emulsion, Soft capsule) |
Antitumor CPM |
Bruceae Fructus* |
Antitumor; (Herb efficacy: Clearing away hot and removing toxin) |
2683 |
Kangai Injection |
Adjuvant antitumor CPM |
Astragali Radix, Ginseng Radix Et Rhizoma, Sophorae Flavescentis Radix |
Tonifying Qi and strengthening body resistance |
2515 |
Fufangbanmao Capsule |
Antitumor CPM |
Mylabris*, Ginseng Radix Et Rhizoma, Astragali Radix, Acanthopanacis Senticosi Radix Et Rhizoma Seu Caulis, Sparganii Rhizoma, Scutellariae Barbatae Herba, Curcumae Rhizoma, Corni Fructus, Ligustri Lucidi Fructus, fel ursi, Glycyrrhizae Radix |
Relieving blood stasis, resolving stagnation, removing toxin, and corroding sores |
2098 |
Zhenqifuzheng Granule (Capsule, Tablet) |
Adjuvant antitumor CPM |
Astragali Radix, Ligustri Lucidi Fructus |
Tonifying Qi and nourishing yin |
1871 |
Huachansu Injection (Capsule, Tablet) |
Antitumor CPM |
Bufonis Corium* |
Removing toxin, detumescence, and relieving pain |
1387 |
Xiaoaiping Injection (Oral formulations) |
Antitumor CPM |
Marsdenia tenacissima Caulis |
Antitumor, anti-inflammatory, and antiasthmatic |
1339 |
Fufangzaofan Pill |
Adjuvant antitumor CPM |
Melanteritum, Panacis Quinquefolii Radix, Hippocampus, Cinnamomi Cortex, Jujubae Fructus, Juglandis Semen |
Warming kidney, tonifying marrow, Qi, yin and blood, and stanching bleeding |
1191 |
Huangqi Injection |
Adjuvant antitumor CPM |
Astragali Radix |
Tonifying Qi and strengthening body resistance, pulse-invigorating and heart-nourishing, fortifying spleen and disinhibiting dampness |
943 |
Pingxiao Capsule (Tablet) |
Antitumor CPM |
Curcumae Radix, Agrimoniae Herba, Trogopterori Faeces, Alumen, Nitrum, Toxicodendri Resina*, Aurantii Fructus, Strychni Semen Pulveratum* |
Promoting blood circulation for removing blood stasis, relieving pain, resolving mass, clearing away hot, removing toxin, strengthening body resistance, and eliminating pathogen |
762 |
Kanglaite Injection (Soft Capsule) |
Antitumor CPM |
Jobstears Seed Oil |
Tonifying Qi, nourishing yin, and resolving mass |
628 |
Fermental Preparation of Chongcaojun |
Adjuvant antitumor CPM |
Cordyceps |
Supplementing lung and kidney, and tonifying essence Qi |
624 |
Yixuesheng Capsule |
Adjuvant antitumor CPM |
Asini Corii Colla, Testudinis Carapacis et Plastri Colla, Cervi Cornus Colla, Deer blood, Beef marrow, Hominis Placenta, Cervi Cornu Pantotrichum, Poria, Astragali Radix Praeparata Cum Melle, Paeoniae Radix Alba, Polygoni Multiflori Radix Praeparata, Jujubae Fructus, Crataegi Fructus, Hordei Fructus Germinatus, Galli Gigerii Endothelium Corneum, Anemarrhenae Rhizoma, Rhei Radix et Rhizom, Testa Arachidis |
Spleen invigorating and kidney nourishing, replenishing blood, supplying essences |
548 |
*Toxic materials indicated in China's Pharmacopoeia or literature.
We noticed that CPMs in two NBMIDC subcategories have overlapping raw materials. For example, in top 15 anticancer CPMs, five adjuvant antitumor CPMs and two antitumor CPMs (Aidi Injection and Fufangbanmao Capsule) has a herb material Huang-Qi (Astragali Radix). Both an antitumor CPM (Fufangkushen Injection) and an adjuvant antitumor CPM (Kangai Injection) contain the herb Ku-Shen (Sophorae Flavescentis Radix). These CPMs showed similar applicable indications (Fig. 2). Moreover, five antitumor CPMs including Aidi Injection and Fufangbanmao Capsule contain toxic materials indicated in China's Pharmacopoeia or literature (Table 1), which may reflect the TCM idea of “fighting poison with poison”.
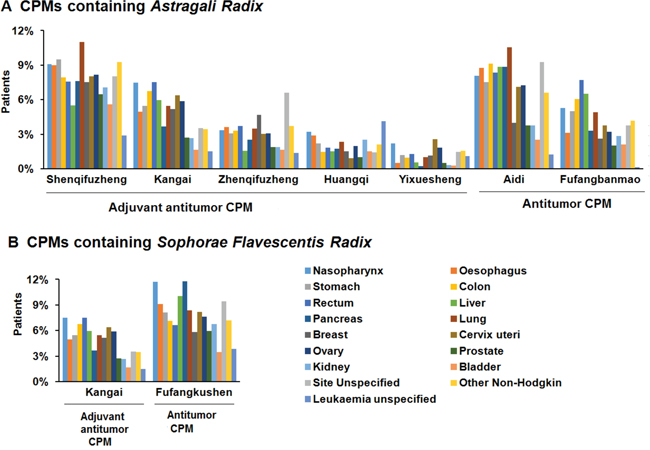
Figure 2: Use frequency of seven CPMs containing Astragali Radix (A) and two CPMs containing Sophorae Flavescentis Radix (B) that in both “antitumor” and “adjuvant antitumor” subcategories of CPM.
Cancer profile of anticancer CPMs and WMs by bi-clustering analysis
Anticancer CPMs tended to be used for a broad spectrum of top 17 cancers (Fig. 3A). Few of these (Huaier, Jinlong, Ganfule and Zilongjin) showed selectivity but had a relatively low use rate (<6%) in the specific cancers. The top two frequently used anticancer CPMs (Shenqifuzheng injection and Fufangkushen injection) were used for almost all 17 types of cancers. By contrast, anticancer WMs were more specific in cancer therapy (Fig. 3B). Meanwhile, anticancer WMs for liver and kidney cancers were used at a lower rate than those for other cancers. Table S4 showed 22 anticancer WMs with use frequency more than 500 patients.
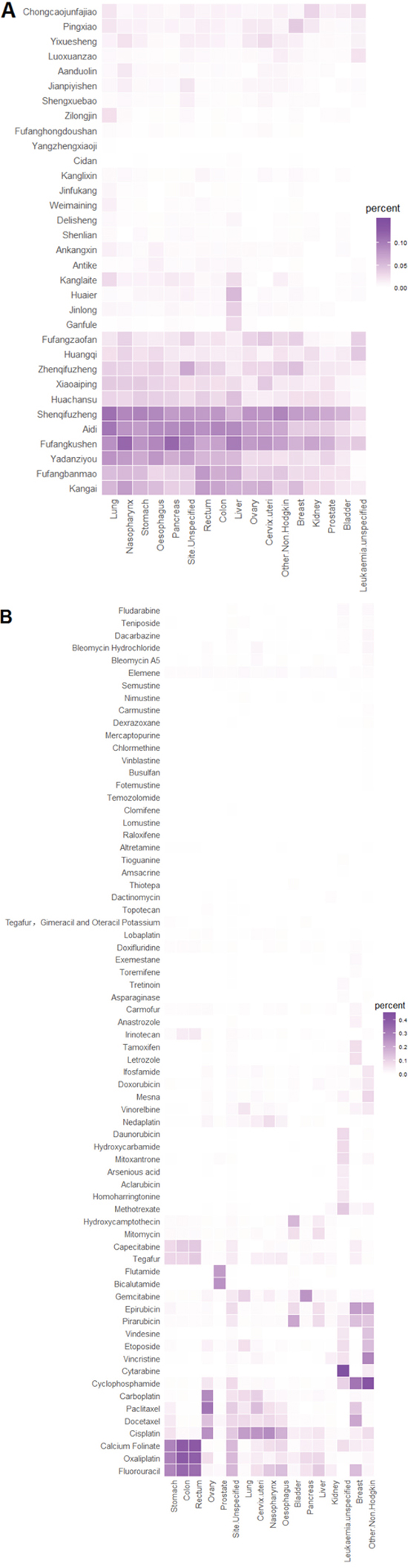
Figure 3: Cancer profiles of anticancer CPMs (A) and anticancer WMs (B).
Individual anticancer medicines for top 17 cancers
Individually, anticancer CPMs do not dominate the cancer therapy. The top use rate of individual anticancer CPMs in 17 cancers except liver and kidney cancers was much lower than that of anticancer WMs (Table 2). The highest use rate of the CPMs in 17 cancers was Fufangkushen injection in nasopharynx and pancreas cancers (12%), a value much lower than that of individual anticancer WMs (45% for Cytarabine in leukaemia unspecified). Furthermore, the most commonly used WM for stomach cancer was a regimen of Oxaliplatin/Fluorouracil/LV, whereas the NCCN guideline (Version 1.2008) recommended 5-FU, Capecitabine, ECF (Epirubicin/Cisplatin/Fluorouracil) or DCF (Docetaxel/Cisplatin/Fluorouracil), based on high-level evidence. The top two anticancer WMs commonly used for bladder cancer (Pirarubicin and Hydroxycamptothecin) in current data were absent in NCCN guideline (Version 1.2008).
Table 2: 17 cancers (>500 patients) and the top used anticancer medicines
Cancer |
Top 3 commonly used anticancer CPMs (use rate, %) |
Top 3 commonly used anticancer WMs (use rate, %) |
||||
|---|---|---|---|---|---|---|
Nasopharynx |
Fufangkushen (12%) |
Shenqifuzheng (9.1%) |
Aidi (8.1%) |
Cisplatin (26%) |
Fluorouracil (12%) |
Docetaxel (8.7%) |
Oesophagus |
Fufangkushen (9.1%) |
Shenqifuzheng (9.0%) |
Aidi (8.8%) |
Cisplatin (18%) |
Fluorouracil (15%) |
Calcium Folinate (8.9%) |
Stomach |
Shenqifuzheng (9.5%) |
Fufangkushen (8.1%) |
Aidi (7.5%) |
Oxaliplatin (29%) |
Calcium Folinate (28%) |
Fluorouracil (27%) |
Colon |
Aidi (9.1%) |
Shenqifuzheng (7.9%) |
Fufangkushen (7.1%) |
Oxaliplatin (39%) |
Calcium Folinate (39%) |
Fluorouracil (35%) |
Rectum |
Aidi (8.4%) |
Fufangbanmao (7.7%) |
Shenqifuzheng (7.6%) |
Calcium Folinate (40%) |
Oxaliplatin (37%) |
Fluorouracil (33%) |
Liver |
Fufangkushen (10%) |
Aidi (8.8%) |
Fufangbanmao (6.5%) |
Fluorouracil (12%) |
Oxaliplatin (8.9%) |
Pirarubicin (7.6%) |
Pancreas |
Fufangkushen (12%) |
Aidi (8.9%) |
Shenqifuzheng (7.6%) |
Gemcitabine (25%) |
Oxaliplatin (8.7%) |
Fluorouracil (6.1%) |
Lung |
Shenqifuzheng (11%) |
Aidi (11%) |
Fufangkushen (8.4%) |
Cisplatin (22%) |
Gemcitabine (10%) |
Docetaxel (8.7%) |
Breast |
Shenqifuzheng (7.5%) |
Fufangkushen (5.8%) |
Kangai (5.2%) |
Cyclophosphamide (32%) |
Epirubicin (22%) |
Docetaxel (20%) |
Cervix uteri |
Fufangkushen (8.2%) |
Shenqifuzheng (8.0%) |
Aidi (7.1%) |
Cisplatin (24%) |
Paclitaxel (15%) |
Carboplatin (11%) |
Ovary |
Shenqifuzheng (8.2%) |
Fufangkushen (7.6%) |
Aidi (7.3%) |
Paclitaxel (32%) |
Carboplatin (27%) |
Cisplatin (25%) |
Prostate |
Shenqifuzheng (6.5%) |
Fufangkushen (6.0%) |
Aidi (3.7%) |
Bicalutamide (25%) |
Flutamide (23%) |
Docetaxel (22%) |
Kidney |
Shenqifuzheng (7.1%) |
Fufangkushen (6.8%) |
Aidi (3.8%) |
Fluorouracil (4.1%) |
Vincristine (3.5%) |
Gemcitabine (2.5%) |
Bladder |
Shenqifuzheng (5.6%) |
Fufangkushen (3.5%) |
Aidi (2.5%) |
Pirarubicin (20%) |
Hydroxycamptothecin (16%) |
Epirubicin (8.2%) |
Site Unspecified |
Fufangkushen (9.4%) |
Aidi (9.0%) |
Shenqifuzheng (8.0%) |
Fluorouracil (16%) |
Oxaliplatin (16%) |
Calcium Folinate (16%) |
Other Non-Hodgkin |
Shenqifuzheng (9.3%) |
Fufangkushen (7.2%) |
Aidi (6.6%) |
Cyclophosphamide (43%) |
Vincristine (28%) |
Epirubicin (20%) |
Leukaemia unspecified |
Huangqi (4.1%) |
Fufangkushen (3.9%) |
Fufangzaofan (3.4%) |
Cytarabine (45%) |
Methotrexate (12%) |
Cyclophosphamide (10%) |
Table 3 illustrates the mean and maximum use rate of anticancer CPMs and WMs in top 17 cancers, respectively. The coefficient of the variation (CV) value, characterizing the extent of variability of the use rate of anticancer CPMs, ranged from 24% to 93%, with a mean of 49%. This result was significantly lower than that of anticancer WMs, which ranged from 97% to 255%, with a mean of 152%. The results once again indicated less selectivity of anticancer CPMs in cancer therapy.
Table 3: Use rate of individual anticancer medicine in 17 cancers (> 500 patients)
Drugs |
Category |
Maximum rate (cancer) |
Use rate in 17 cancers |
||
|---|---|---|---|---|---|
Mean |
CV |
Mean of CV |
|||
Shenqifuzheng |
CPM |
11.0% (Lung) |
7.7% |
24% |
49% |
Fufangkushen |
CPM |
11.8% (Pancreas) |
7.7% |
30% |
|
Aidi |
CPM |
10.6% (Lung) |
6.8% |
40% |
|
Kangai |
CPM |
7.5% (Rectum) |
4.7% |
40% |
|
Yadanziyou |
CPM |
8.2% (Lung) |
4.5% |
57% |
|
Fufangbanmao |
CPM |
7.7% (Rectum) |
3.9% |
48% |
|
Zhenqifuzheng |
CPM |
6.6% (Site Unspecified) |
3.1% |
42% |
|
Huachansu |
CPM |
4.7% (Liver) |
2.5% |
43% |
|
Xiaoaiping |
CPM |
4.1% (Cervix uteri) |
2.5% |
46% |
|
Fufangzaofan |
CPM |
4.1% (Cervix uteri) |
2.2% |
51% |
|
Huangqi |
CPM |
4.1% (Leukaemia unspecified) |
2.0% |
41% |
|
Pingxiao |
CPM |
3.9% (Breast) |
1.3% |
61% |
|
Kanglaite |
CPM |
2.8% (Lung) |
0.9% |
93% |
|
Chongcaojunfajiao |
CPM |
3.1% (Kidney) |
1.2% |
57% |
|
Yixuesheng |
CPM |
2.6% (Cervix uteri) |
1.1% |
61% |
|
Fluorouracil |
WM |
34.9% (Colon) |
11.4% |
99% |
152% |
Oxaliplatin |
WM |
39.2% (Colon) |
10.0% |
127% |
|
Calcium Folinate |
WM |
39.6% (Rectum) |
10.0% |
129% |
|
Cisplatin |
WM |
26.2% (Nasopharynx) |
9.8% |
97% |
|
Cyclophosphamide |
WM |
42.6% (Other Non-Hodgkin) |
6.2% |
196% |
|
Docetaxel |
WM |
20.2% (Breast) |
4.9% |
118% |
|
Paclitaxel |
WM |
31.9% (Ovary) |
5.5% |
152% |
|
Epirubicin |
WM |
22.2% (Breast) |
4.6% |
149% |
|
Pirarubicin |
WM |
20.0% (Bladder) |
4.3% |
136% |
|
Carboplatin |
WM |
26.5% (Ovary) |
3.7% |
176% |
|
Gemcitabine |
WM |
24.6% (Pancreas) |
3.7% |
159% |
|
Tegafur |
WM |
11.7% (Rectum) |
3.5% |
103% |
|
Capecitabine |
WM |
12.2% (Rectum) |
2.8% |
144% |
|
Etoposide |
WM |
14.7% (Other Non-Hodgkin) |
2.3% |
168% |
|
Vinorelbine |
WM |
5.8% (Lung) |
1.3% |
144% |
|
Vincristine |
WM |
27.6% (Other Non-Hodgkin) |
2.6% |
255% |
|
Nedaplatin |
WM |
7.5% (Nasopharynx) |
1.4% |
150% |
|
Mitomycin |
WM |
7.4% (Bladder) |
1.4% |
158% |
|
Hydroxycamptothecin |
WM |
16.2% (Bladder) |
1.7% |
221% |
|
Irinotecan |
WM |
5.0% (Rectum) |
0.9% |
169% |
|
Combined use networks of anticancer CPMs and WMs
In this survey, a total of 12,743 (24.8%) patients used both anticancer CPMs and WMs simultaneously during their hospital stays. To obtain the combined use patterns of both medicines, a CPM-WM combined use network for four major cancers in China was constructed (Fig. 4). Among the high frequent combinations, adjuvant antitumor CPMs were more commonly used in conjunction with WMs in treating lung cancer. The gastrointestinal cancers, in particular stomach and colorectal cancers, shared similar combination profiles, in which CPMs tended to band together with the first line WM regimens, such as FOLFOX4. Meanwhile, adjuvant antitumor CPMs including Shenqifuzheng injection and antitumor CPMs including Aidi injection were involved in all four cancers together with WMs. Parts of these CPM-WM combinations were supported by clinical evidence as reported (Table S5).
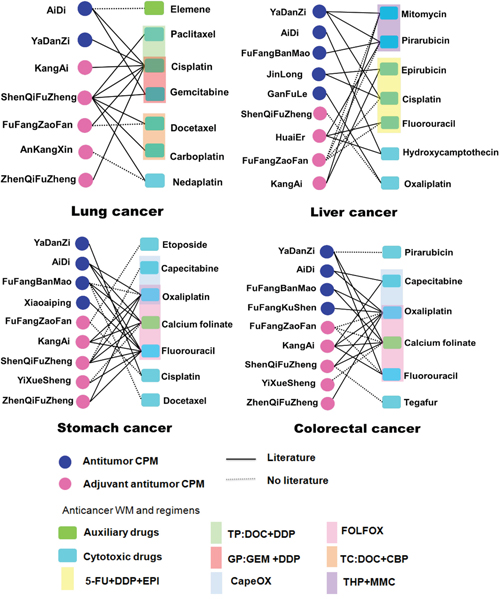
Figure 4: Combined use network of anticancer CPMs and WMs in four major cancers. The combined links in networks marked with the full lines were supported by clinical evidence (Table S5), and those with the dotted lines lacked clinical reports.
DISCUSSION
This nationwide analysis characterizes how CPMs are used to fight cancer in China. In general, anticancer CPMs have gained increased popularity and been used in almost half (42.4%) of investigated cancer patients. The cost per patient for all anticancer CPMs is lower than that of anticancer WMs. We found that CPMs with less raw materials are relatively more popular in treating cancers (Fig. 1; Table S3). This is partly due to CPM injections that usually composed of less raw materials are used more commonly than other CPMs. And the less raw materials may make the CPMs easier to understand and more acceptable for clinicians. Compared with 71 anticancer WMs, the use rate of 33 anticancer CPMs was higher than in liver, kidney, pancreatic, and esophagus cancers. There are two probable reasons. Firstly, these four cancers may have less specific and effective anticancer WMs than other cancers, leading to a lower use rate of anticancer WMs. Secondly, some first line drugs for the liver cancer and kidney cancer such as Sorafenib and Sunitinib were not covered by NBMIDC, making the use rate of anticancer WMs much lower in liver cancer (29%) and kidney cancer (17%). By contrast, the anticancer CPMs are widely used in various cancers, and thus showing a relatively higher rate in these four cancers especially in liver and kidney cancers.
In this study, a “widespread and dispersive” charateristic with low selectivity for the use of anticancer CPMs has been revealed (Table 2, Table 3 and Fig. 3). Although the mean usage of anticancer CPMs was significantly higher than their western counterparts, the use rates of top anticancer CPMs (no more than 12%) were much lower than those of top WMs (a maximum of 45%) in 17 main cancers except kidney cancer (Table 2). The results suggest the individual anticancer CPMs are not dominant in a specific cancer treatment. One possible reason is that CPMs always regulate overall health of human body rather than simply fight against a specific cancer. A typical case is Shenqifuzheng injection, the most often used adjuvant antitumor CPM. This injection, broadly used for almost all 17 cancers, is composed of Huang-Qi (Astragali Radix) and Dang-Shen (Codonopsis Pilosula). Both of the two herbs contain immunomodulatory ingredients, and can improve the immune function of cancer patients receiving chemotherapy [11–14]. Thus, Shenqifuzheng injection could be widely used as an efficacious adjuvant to prevent immunity impairment that usually occurs in therapy of various cancers. Another reason for the low selectivity of CPMs is that the precise efficacy of CPMs is not quite clear in clinical use. Anticancer CPMs mainly labeled their traditional efficacy (Table 1). However, the applicable cancer type was not clearly stated in instructions or just indicated as “et al.” or “advanced cancers” for many CPMs. Thus, the specific and evidence-based indications are still required to improve the rational use of CPMs. This study also indicates the subcategory classification of CPMs in NBMIDC needs to be further clarified, since both CPM subcategories have similar clinical use patterns and overlapped herb materials such as Astragali Radix (an immunomodulatory herb [11, 12]) and Sophorae Flavescentis Radix (an anti-tumor herb [15, 16]) (Fig. 2). Special safety caution should also be paid to CPM injections and CPMs containing toxic ingredients.
The CPMs and WMs are commonly used in combination and work in concert for cancer treatment. Most of the herb-drug pairs identified by our network analysis (Fig. 4) have clinical evidence (Table S5), often reported as improving quality of life of patients and reducing adverse reactions of chemotherapy. Thus, CPMs may offer potential therapeutic benefits for cancer patients by boosting efficiency and decreasing toxicity caused by WMs. Other herb-drug pairs lacking of references deserve further investigation. More solid evidence and whether new safety risks can be generated from the herb-drug interactions needs further studies. A standard program will be of great significance to guide the combined use of CPMs and WMs.
Although our data only catch sampled patients in China and the results need to be validated in larger samples, this analysis for the first time addressed the clinical use of anticancer CPMs in a China nationwide. This study provides valuable information to improve the standardization, rationalization and internationalization of the clinical use of Chinese medicines.
MATERIALS AND METHODS
National-wide sampling
Data was from a nationwide survey for inpatients' utilization of health services covered by China's urban basic medical insurance from 2008 to 2010. All patients were firstly sorted by discharge time and then randomly sampled from China's 29 provincial-level administrative regions. The inpatients came from 2,576 hospitals in 22 provinces, 3 autonomous regions, and 4 centrally-administered municipalities. The percentage of the sampled inpatients who had medical insurance coverage was 2% in the centrally-administered municipalities and provincial capitals, 5% in the prefecture-level cities, and 10% in the counties.
Drugs and cancer patients' data
The drugs, medication records and cost for 51,382 malignant tumor inpatients, including 11209 cases (21.8%) in 2008, 16850 cases (32.8%) in 2009, and 23323 cases (45.4%) in 2010, were retrieved from the sampling data. The data on two types of drugs were collected, including CPMs (registered and approved by China State Food and Drug Administration) and WMs (all modern medicines including saline, glucose and other auxiliary drugs).
NBMIDC recorded anticancer CPMs and WMs
A total of NBMIDC-covered 33 anticancer CPMs (calculated by the number of generic names after different dosage forms were merged) and 71 anticancer WMs (calculated by the number of generic names of the active pharmaceutical ingredients) were used in sampled cancer patients. For anticancer CPMs, 17 fall into the NBMIDC “Antitumor” subcategory and 16 into the “Adjuvant antitumor” subcategory. The number of raw materials (herbs, animals or others) contained in each anticancer CPMs ranges from 1 to 22, and 124 materials get involved. Anticancer WMs include 56 cytotoxic, 9 hormone, 4 auxiliary and 2 other drugs.
Statistical, bi-clustering, and network analysis
Use-frequency of a drug (CPM or WM) refers to the total number of patients in which a drug was used in the medication records. Use rate of a drug was the percentage of the total cancer patients or patients with a specific cancer who used the drug. Cost ratio means Ratio of the total drug cost. A Mann-Whitney rank sum test was used to evaluate the statistical significance of the use rate and cost between the anticancer CPMs and anticancer WMs, as well as a comparison analysis for different types of anticancer CPMs. A Spearman rank correlation analysis was used to analyze the correlation between the rank of use rates and the rank of number of raw materials contained in each anticancer CPMs.
Bi-clustering method was used to analyze the cancer profile of anticancer CPMs and WMs. A bipartite graph was first created for drugs and various types of cancers, in which nodes denoted drugs or cancers, and edges denoted the use of a drug for a particular cancer. The weights of edges were expressed as the use rate of drug, which represented the percentage of patients with a certain cancer who used drug. Then, hierarchical clustering was performed for drugs using all of the row vectors to cluster together similar drugs. Similarly, hierarchical clustering was performed for the various types of cancers to cluster together similar cancers. The order of drugs and cancers was adjusted according to the results of the clustering and a heat map was generated.
A network approach was used to analyze the combined use of CPMs and WMs [17]. The network nodes represented drugs, and the edges represented the combined relationship between two drugs. The combined relationship was measured by two indicators. One was the frequency of the combined use, which referred to the number of cancer patients who used drugs in combination. The other was the mutual information entropy [17]. The effective combined relationships were screened (total number of combined use >50 times, or total combined mutual information >0.005) for constructing CPM-WM combined use networks (see Supplementary text).
ACKNOWLEDGMENTS
We thank China Health Insurance Research Association affiliated with the Ministry of Human Resources and Social Security of China for providing data.
GRANT SUPPORT
This work is partly supported by National Natural Science Foundation of China (81225025 and 91229201).
CONFLICTS OF INTEREST
There are no conflict of interest disclosures from any authors.
REFERENCES
1. Normile D. Asian medicine: The new face of traditional Chinese medicine. Science. 2003; 299:188–190.
2. Ministry of Human Resources and Social Security of the People’s Republic of China. China’s National Basic Medical Insurance, Work Injury Insurance and Maternity Insurance Drugs Catalog (2009 edition). China Labour and Social Security Publishing House. 2009; 12–1.
3. Tong B, Ding N, Wei Q. Analysis of the Utilization of Antineoplastic Agents in Our Hospitals during the Period of 2009–2011. China Pharmacy. 2012; 23:3960–3963.
4. Wang J, Lu M, Zhang G, Lu H. Utilization of Antitumor Drugs in Changshu Hospital Affiliated to Soochow University during 2010–2013. Evaluation and analysis of drug-use in hospitals of China. 2014; 14:908–912.
5. Xu Y, Wang X, Luan W. Analysis on Drug Use in PLA General Hospital During 2008–2010. Evaluation and analysis of drug-use in hospitals of China. 2012; 12:109–113.
6. Wang CY, Bai XY, Wang CH. Traditional Chinese medicine: a treasured natural resource of anticancer drug research and development. Am J Chin Med. 2014; 42:543–59.
7. Liang X, Li H, Li S. A novel network pharmacology approach to analyse traditional herbal formulae: the Liu-wei-di-huang Pill as a case study. Molecular BioSystems. 2014; 10:1014–1022.
8. Adepoju L, Wanjiku S, Brown M, Qu W, Williams M, Redfern RE, Sferra JJ. Effect of insurance payer status on the surgical treatment of early stage breast cancer: data analysis from a single health system. JAMA Surg. 2013; 148:570–2.
9. Robbins AS, Pavluck AL, Fedewa SA, Chen AY, Ward EM. Insurance status, comorbidity level, and survival among colorectal cancer patients age 18 to 64 years in the National Cancer Data Base from 2003 to 2005. J Clin Oncol. 2009; 27:3627–33.
10. Chen W, Zhang S, Zheng R, Zeng H, Zou X, Zhao P, Wu L, Li G, Hao J. Report of Cancer Incidence and Mortality in China, 2009. China Cancer. 2013; 22:2–12.
11. Kang H, Ahn KS, Cho C, Bae HS. Immunomodulatory effect of Astragali Radix extract on murine TH1/TH2 cell lineage development. Biol Pharm Bull. 2004; 27:1946–50.
12. Lee YS, Han OK, Park CW, Suh SI, Shin SW, Yang CH, Jeon TW, Lee ES, Kim KJ, Kim SH, Yoo WK, Kim HJ. Immunomodulatory effects of aqueous-extracted Astragali radix in methotrexate-treated mouse spleen cells. J Ethnopharmacol. 2003; 84:193–8.
13. Zeng XL, Li XA, Zhang BY. Immunological and hematopoietic effect of Codonopsis pilosula on cancer patients during radiotherapy. Zhongguo Zhong Xi Yi Jie He Za Zhi. 1992; 12:607–8. 581.
14. Zhuang SR, Chen SL, Tsai JH, Huang CC, Wu TC, Liu WS, Tseng HC, Lee HS, Huang MC, Shane GT, Yang CH, Shen YC, Yan YY, Wang CK. Effect of citronellol and the Chinese medical herb complex on cellular immunity of cancer patients receiving chemotherapy/radiotherapy. Phytother Res. 2009; 23:785–790.
15. Wang Z, Zhang J, Wang Y, Xing R, Yi C, Zhu H, Chen X, Guo J, Guo W, Li W, Wu L, Lu Y, Liu S. Matrine, a novel autophagy inhibitor, blocks trafficking and the proteolytic activation of lysosomal proteases. Carcinogenesis. 2013; 34:128–138.
16. Xie SB, He XX, Yao SK. Matrine-induced autophagy regulated by p53 through AMP-activated protein kinase in human hepatoma cells. Int J Oncol. 2015; 47:517–26.
17. Li S, Zhang B, Jiang D, Wei YY, Zhang NB. Herb network construction and co-module analysis for uncovering the combination rule of traditional Chinese herbal formulae. BMC Bioinformatics. 2010; 11:S6.