
Introduction
Lung cancer in Canada is one of the most common solid malignancies in North America. It holds a poor prognosis, with an average 5-year survival of less than 19% for all-comers [1]. Accurately diagnosing, prognosticating, monitoring, and treating lung cancer is crucial to lung cancer management. Currently, disease quantification and monitoring rely heavily on radiographic and clinical assessment, and there remain few widely used biochemical tools to assist in this evaluation. Newer technologies such as ctDNA have started to transform the landscape of minimally invasive techniques that can facilitate cancer screening and early diagnosis, enhance prediction and prognostication, correlate with staging, profile cancer-associated mutations and genomic alterations, and monitor for treatment response and resistance [2]. However, such technologies still have a number of hurdles to overcome before they are readily adopted into widespread clinical practice, of which cost is one [3, 4].
To date, a number of studies have explored the utility of readily available, low-cost tumour biomarkers in the assessment and management of NSCLC, spanning the breadth of screening [5], diagnosis and staging [6, 7], prognostication [8–19], prediction [13, 20–24], and monitoring/surveillance [13, 25–28]. However, most have been specific to a particular disease stage and/or treatment, or reported biomarker level measurements at only a single timepoint for their association with clinical or radiographic features. Furthermore, recent international NSCLC guidelines offer either no recommendations on the utility of conventional serum tumor markers in disease management, or do not suggest their use altogether [29–34]. However, the evidence for these recommendations is weak. Thus, there is clearly an unmet need for further exploration of their application in this disease space.
The aim of this retrospective study was to provide additional evidence for the clinical use of conventional serum tumor markers CEA, CA19-9, and CA-125 in NSCLC management. These markers have been analyzed in similar contexts as cited above, were reliably accessible at the index institution at the time of study, and are widely available in clinical settings for measurement. Results of this research are positioned to provide further support for their application in NSCLC.
Results
A total of 533 NSCLC patients were identified for screening at London Health Sciences Centre, London, Ontario, Canada. 165 patients met inclusion criteria for Cohort A, and 92 patients for Cohort B. Patients were most commonly excluded due to failing to meet tumor marker and/or imaging investigation measurement within the timeframes detailed in the Methods section above. Baseline demographics between Cohort A and B were similar (Table 1). In cohort A, patients most commonly had stage IV disease (69.7%), adenocarcinoma histology (77.0%), and had a median age of 65 years. At baseline 58.8% of patients had an elevated CEA >ULN, 50.9% had CA-125 >ULN, and 30.3% had CA19-9 >ULN (Table 1). Figure 1 demonstrates the distribution of elevated tumor markers patients in Cohort A who had at least one marker above the ULN at baseline.
Table 1: Baseline demographics of patients in Cohort A (n = 165; baseline tumor markers only) and Cohort B (n = 92; paired tumor markers and radiographic scans)
| Cohort A | Cohort B | Cohort A | Cohort B | Cohort A | Cohort B | |||
|---|---|---|---|---|---|---|---|---|
| Chemotherapy | Histologic subtype | Stage | ||||||
| Yes | 55.2% | 65.2% | Adenocarcinoma | 77.0% | 77.2% | I | 1.2% | 1.1% |
| No | 43.6% | 34.8% | Squamous cell | 16.4% | 17.2% | II | 2.4% | 2.2% |
| Radiation | Large Cell | 0.6% | 1.1% | III | 24.2% | 35.9% | ||
| Yes | 38.8% | 43.5% | Other/Missing | 6.0% | 4.4% | IV | 69.7% | 59.8% |
| No | 60.0% | 56.5% | Sex | Elevated biomarker at baseline (>ULN) | ||||
| Immunotherapy | Male | 50.9% | 46.7% | CEA | 58.8% | 54.3% | ||
| Yes | 35.2% | 46.7% | Female | 49.1% | 53.3% | CA-125 | 50.9% | 46.7% |
| No | 63.6% | 56.5% | Age | CA19-9 | 30.3% | 22.8% | ||
| Surgery | Median | 66 | 64 | |||||
| Yes | 4.8% | 3.3% | ||||||
| No | 93.9% | 96.7% | ||||||
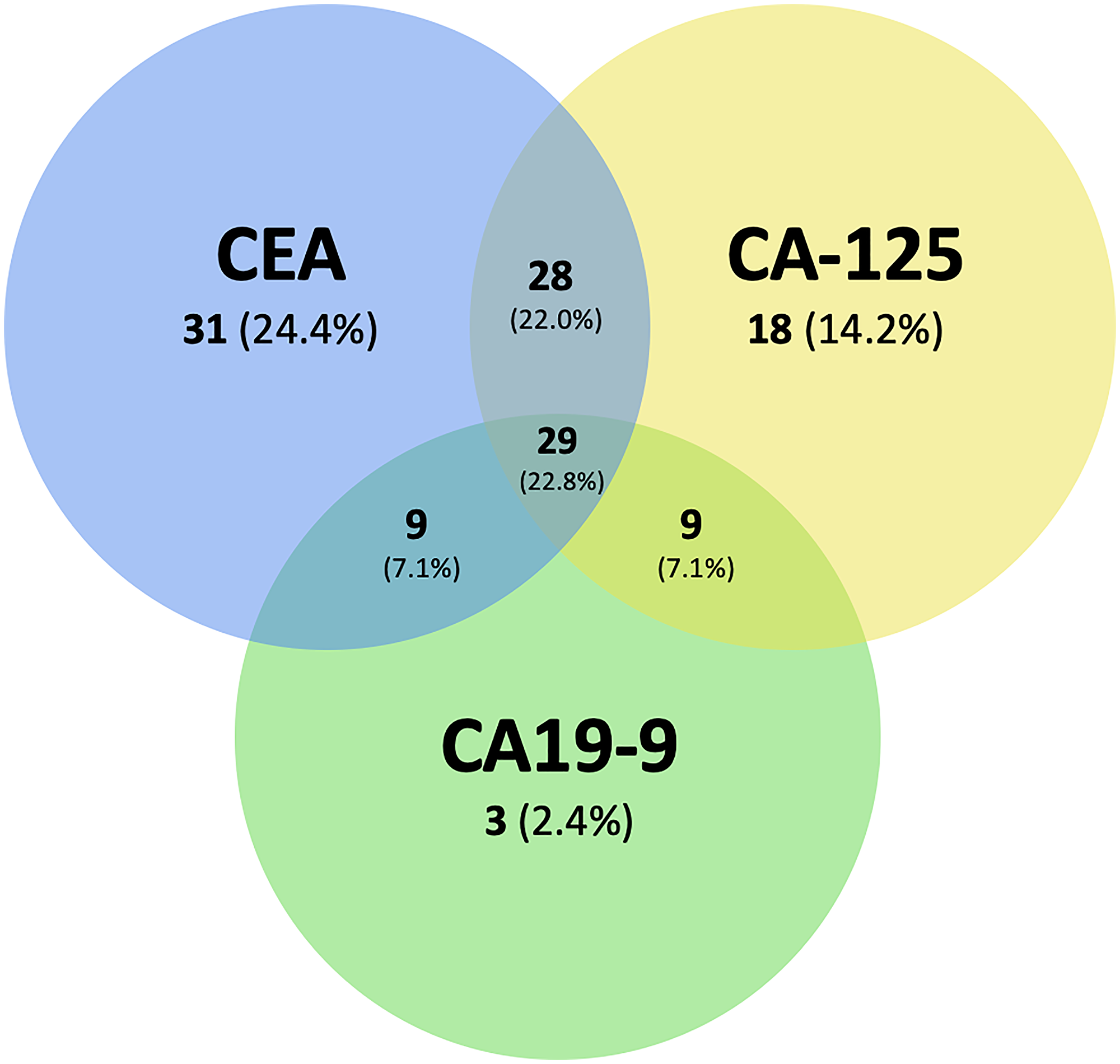
Figure 1: Venn diagram of the distribution of number of patients with elevated tumor markers who had at least one marker above the ULN at baseline (ULN) in Cohort A.
Overlaps represent combinations of elevated tumor markers elevated above the ULN at baseline. Percentages represent the fraction of patients in each subgroup relative to those with at least one tumor marker elevated above the ULN at baseline.
In Cohort A, demographic and clinical characteristics were analyzed for their association with elevated CEA at baseline. Adenocarcinoma was more likely to be associated with a CEA >ULN at baseline (Risk Ratio (RR) 1.36, 95% CI 1.12–1.66, p < 0.001), and squamous cell carcinoma was less likely (RR 0.29, 95% CI 0.14–0.63, p < 0.001). Stage III disease was less likely to be associated with CEA >ULN at baseline (RR 0.70, 95% CI 0.41–1.20, p < 0.001), while stage IV disease was more likely (RR 1.27, 95% CI 1.01–1.58, p < 0.001). Tumor EGFR or KRAS mutation statuses were not associated with an elevated CEA at baseline (EGFR RR 1.00, 95% CI 0.88–1.13, p = 0.98; KRAS RR 1.03, 95% CI 0.90–1.18, p = 0.63) (Table 2). In patients with stage IV disease in Cohort A, a survival analysis was completed to determine if there was a relationship with elevated CEA levels at baseline and all-cause mortality. A total of 69 patients (60.0%) of 115 died during follow up. An elevated baseline CEA was not associated with a difference in overall survival (HR 1.05, 95% CI 0.63–1.74, p = 0.84).
Table 2: Associations of demographic features with CEA level above the ULN at baseline for patients in Cohort A (n = 165) analyzed using risk rations
| Variable | Value | Total N | Percent with CEA>5 | Risk ratio | 95% CI | p-value | |
|---|---|---|---|---|---|---|---|
| NSCLC subtype | Adenocarcinoma yes | 127 | 66.1% | 1.36 | 1.12 | 1.66 | <0.001 |
| Adenocarcinoma no | 36 | 33.3% | 1.00 (referent) | ||||
| SCC yes | 27 | 39.6% | 0.29 | 0.14 | 0.63 | <0.001 | |
| SCC no | 136 | 64.7% | 1.00 (referent) | ||||
| Stage | Stage III yes | 40 | 50.0% | 0.70 | 1.41 | 1.20 | <0.001 |
| Stage III no | 125 | 61.6% | 1.00 (referent) | ||||
| Stage IV yes | 115 | 64.3% | 1.27 | 1.01 | 1.58 | <0.001 | |
| Stage IV no | 50 | 46.0% | 1.00 (referent) | ||||
| Mutation | EGFR yes | 22 | 59.1% | 1.00 | 0.88 | 1.13 | 0.98 |
| EGFR no | 143 | 58.7% | 1.00 (referent) | ||||
| KRAS yes | 27 | 63.0% | 1.03 | 0.90 | 1.18 | 0.063 | |
| KRAS no | 138 | 58.0% | 1.00 (referent) | ||||
Cohort B was analyzed for differences in tumor marker levels at response and progression relative to levels at baseline and nadir, respectively. Median (IQR) fold-change in tumor markers from nadir to progression were 2.13 (IQR 1.24–3.02; p < 0.001) for CEA (n = 47), 1.46 (IQR 1.13-2.18; p < 0.001) for CA19-9 (n = 46), and 1.53 (IQR 0.96–2.12; p < 0.001) for CA-125 (n = 47) (Figure 2A). Median (IQR) fold-change in tumor markers from baseline to their level at radiographic response (complete or partial) were 0.50 (IQR 0.27–0.95; p < 0.001) for CEA (n = 39), 1.08 (IQR 0.74–1.61; p = 0.99) for CA19-9 (n = 35), and 0.47 (IQR 0.18–1.26; p = 0.008) for CA-125 (n = 35) (Figure 2B). Thus, all three tumor markers showed significant increases at radiographic progression relative to nadir, and CEA and CA-125 showed significant decreases at radiographic response relative to baseline.
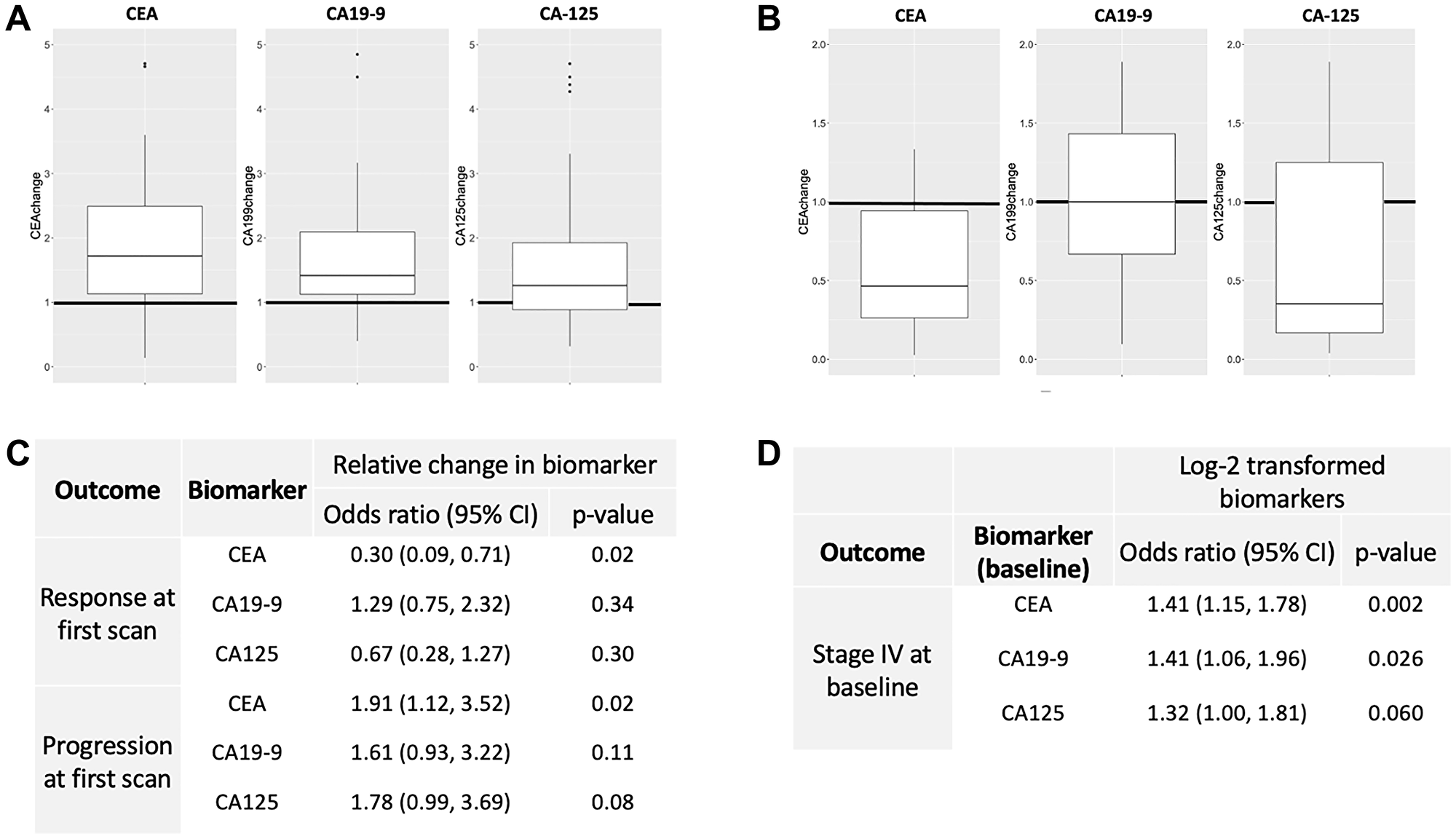
Figure 2: Patients from Cohort B were analyzed.
(A) Box and whisker plots for the median fold-change of CEA, CA19-9, and CA-125 at radiographic progression relative to nadir. All demonstrated statistically significant differences. (B) Box and whisker plots for the media fold-change of CEA, CA19-9, and CA-125 at radiographic response relative to baseline. CEA and CA-125 demonstrated statistically significant differences. (C) Odds ratios for the relative change in each tumor marker level at first follow-up radiographic scan after systemic treatment was initiated. (D) Odds ratios for observing an elevation in biomarker levels at baseline in patients with stage IV disease.
Cohort B was then analyzed for the relative change in tumor marker level at first follow-up radiographic scan after systemic treatment was initiated. Each 100% increase in CEA from baseline to first scan was associated with 70% lower odds of having a response at first scan (OR 0.30, 95% CI 0.09–0.71, p = 0.020) (Figure 2C). Similarly, each 100% increase in CEA from baseline to first scan was associated with 91% higher odds of progression (OR 1.91, 95% CI 1.12–3.52, p = 0.024) at first scan (Figure 2C). Similar associations were not seen for CA19-9 nor CA-125. The presence of stage IV disease did demonstrate significant OR with elevations in CEA and CA19-9 at baseline (Figure 2D). Lastly, using the tumor marker thresholds defined above in the Methods section, sensitivity and specificity for a >25% increase in CEA and radiographic progression were 47.5% and 80.0%, respectively. Sensitivity and specificity were 37.0% and 80%, respectively, for radiographic response.
DISCUSSION
Lung cancer is one of the most common solid tumor diagnoses, and is often associated with a poor prognosis. One minimally invasive tool that can assist in the assessment of NSCLC are conventional tumor biomarkers, with prior studies reporting their utility in screening [5], diagnosis and staging [6, 7], prognostication [8–19], prediction [13, 20–24], and monitoring/surveillance [13, 25–28]. Despite this data, there still remains a lack of consensus around the role that these biomarkers play in disease management, and a paucity of information regarding disease monitoring while on treatment. To help strengthen the evidence base for the use of CEA, CA-125, and CA-19-9 in NSCLC management, this study offers further data to support their use in this setting.
In Cohort A, baseline biomarker levels were assessed for their association with a series of demographic and clinical features (Table 2). Elevated baseline CEA associated with a higher likelihood of stage IV disease and adenocarcinoma histology, the latter or which has been corroborated in at least one other study [35]. No associations with EGFR or KRAS mutation status and expression were found. This contrasted from a prior report [20], however it was restricted to stage IIIB and IV patients and assessed only the role of tyrosine kinase inhibitors in disease management. Lastly, elevated baseline CEA levels in patients with stage IV disease were not associated with overall survival. While this is supported by data from at least one publication [25], others have reported a worse prognosis with higher baseline CEA levels in advanced disease [8, 11, 14]. Thus, important trends are emerging, but unifying the data that already exists will help further contextualize and enhance the findings reported herein.
Importantly, in Cohort B, CEA, CA-125, and CA19-9 all demonstrated significant fold-increases at radiographic progression relative to nadir (Figure 2A). Similarly, CEA and CA-125 were significantly lower than baseline levels for those who responded radiographically (Figure 2B). Relative changes in CEA levels were associated with radiographic progression or response at first follow-up scan (Figure 2C), and the presence of stage IV disease at baseline did associate with elevated CEA and CA19-9 levels (Figure 2D). These important findings offer further support for their use as clinical adjuncts in disease management. Specific applications may include increasing the pre-test probability of disease progression/response on imaging scans when there is radiographic equipoise, or when monitoring for disease response/progression when access to imaging investigations is either delayed or unavailable. These results were found to be statistically significant in a patient population encompassing a wide cross-section of disease histologies, stages, and treatment types.
As with all studies, limitations in methodology and analysis did exist. First, patients selected for tumor marker measurement were not standardized. Ordering of serum CEA, CA-125, and CA19-9 was not standard of care at London Health Sciences Centre at the time of data collection, which could have led to selection bias. Additionally, patients were analyzed from all stages and histologies, but there was a significant over-representation of stage III and IV patients. Thus, applying the conclusions drawn to stage I and II disease may not be clinically appropriate, and should be interpreted with caution. And lastly, sensitivity and specificity using the pre-specified tumor marker change cutoffs were modest. A similar specificity of 70% has been reported in a meta-analysis of six trials studying outcomes of NSCLC patients while on treatment [36], but improved standardization of data collection and broader planned subgroup analyses would likely lead to enhanced sensitivity and specificity.
Notwithstanding the aforementioned limitations, between the pre-existing literature around conventional tumor markers in NSCLC and the results found in this study, there is ample evidence to suggest a need to further explore the clinical utility of these tools. One method would be through a prospective clinical trial, which allows for structured tumor marker data collection with a more homogeneous dataset, reducing bias and enhancing statistical validity. For example, in this study baseline imaging was permitted up to 60 days prior to therapy initiation, which could have led to the first on-treatment scan falsely identifying progression; a prospective study would allow for scheduled measurement of tumor marker levels that would limit this bias. It could also provide data about lead-times that would analyze for prediction of response/progression based on tumor marker changes, for which there exists preliminary supporting data from prior research [25, 27, 28, 37, 38]. Lastly, pre-specified subgroup analyses as well as the study of other biomarkers such as CYFRA21-1, NSE, and CA15-3 could also be completed. In addition to a prospective trial, with the wealth of information that exists in the literature, a meta-analysis would provide a high level of evidence to support the use of these conventional tumor markers in routine clinical care.
In conclusion, these inexpensive, widely available tests with rapid turnaround times and relatively short half-lives (CEA, CA-125, and CA19-9) are perfectly situated to serve as adjunctive clinical tools in the management of NSCLC. They are uniquely positioned to add value to patient care, especially in settings where ctDNA monitoring may not be available.
Materials and Methods
This study was a retrospective single-center review of patients treated at the London Regional Cancer Program in Ontario, Canada. Patients must have had a biopsy-proven diagnosis of NSCLC and received systemic treatment by a medical oncologist between January 1, 2016 and August 1, 2020. Patients must have been 18 years of age or older at the time of treatment, and were excluded if they had an active synchronous cancer, or a known concurrent non-cancerous disease that would have directly confounded results. Research Ethics Board approval was obtained before study initiation. All data were de-identified and stored in a secure REDCap database [39]. Demographic information collected for each patient included age, sex, disease stage at the time of treatment, histology, tumor genomic alterations, year and month of death (if known), as well as treatment modalities used during the relevant study window.
Patients included were divided into two cohorts. Cohort A comprised patients with radiographic imaging and tumor markers levels at baseline that were measured within 60 days prior to, or up to 14 days after, the initiation of systemic therapy. Cohort B was a subset of Cohort A, which included patients with paired radiographic imaging and tumor marker levels at both baseline and at least one follow-up time-point. At radiographic progression or response, tumor markers were included if they were drawn within 30 days of the associated scan. Disease progression or response was determined radiographically using RECIST 1.1 [40] or iRECIST [41] criteria. Tumor biomarker upper limits of normal (ULN) were defined as ≤5.0 Eμg/L for CEA; ≤35 U/mL for CA19-9; and ≤35 U/mL for CA-125.
For Cohort A, associations with demographic and clinical characteristics with elevated CEA levels at baseline were directly estimated. Association of elevated baseline CEA and all-cause mortality for those diagnosed at stage IV was assessed with a hazard ratio and its 95% confidence interval, obtained from Cox proportional hazards regression. All two-sided p-values < 0.05 were considered statistically significant. All analyses were performed using R version 4.1.1.
For statistical analyses involving Cohort B, continuous variables were presented using medians (interquartile range (IQR)), and categorical variables were presented using frequencies (percentage). Changes in biomarker levels for responders were analyzed relative to baseline. Changes in biomarker levels at progression were analyzed relative to levels at nadir. Levels at response and progression were compared to baseline/nadir using the Wilcoxon signed rank test, accounting for the paired nature of the data. Fold-changes in biomarkers between baseline and the time of first imaging were also evaluated against disease classification at the time of first imaging. The association between response/progression and biomarker change at the time of first imaging was assessed using logistic regression to obtain odds ratios and their associated 95% confidence intervals. Lastly, the sensitivity and specificity of CEA for at radiographic progression and response were calculated. A threshold for change in CEA was set at a >25% increase from nadir any time prior to progression, and a >25% decrease from baseline to the time of response was set as the threshold for radiographic response. Thresholds were extrapolated from prior studies, as no standards are yet universally defined [13, 26, 28, 37, 38].
CONFLICTS OF INTEREST
Authors have no conflicts of interest to declare.
ETHICAL STATEMENT AND CONSENT
The study was approved by Western University REB, 116683. Individual consent was not needed as it was a retrospective chart review. The bloodwork was collected as standard of care with the local physician.
FUNDING
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
1. STATCAN. Leading causes of death, total population, by age group. Statistics Canada. 2018. Available from; https://www150.statcan.gc.ca/n1//en/type/data?MM=1#tables.
2. Li RY, Liang ZY. Circulating tumor DNA in lung cancer: real-time monitoring of disease evolution and treatment response. Chin Med J (Engl). 2020; 133:2476–85. https://doi.org/10.1097/CM9.0000000000001097. [PubMed].
3. Chaudhuri AA, Chabon JJ, Lovejoy AF, Newman AM, Stehr H, Azad TD, Khodadoust MS, Esfahani MS, Liu CL, Zhou L, Scherer F, Kurtz DM, Say C, et al. Early Detection of Molecular Residual Disease in Localized Lung Cancer by Circulating Tumor DNA Profiling. Cancer Discov. 2017; 7:1394–403. https://doi.org/10.1158/2159-8290.CD-17-0716. [PubMed].
4. Crosby D. Delivering on the promise of early detection with liquid biopsies. Br J Cancer. 2022; 126:313–15. https://doi.org/10.1038/s41416-021-01646-w. [PubMed].
5. Triphuridet N, Vidhyarkorn S, Worakitsitisatorn A, Sricharunrat T, Teerayathanakul N, Auewarakul C, Chungklay N, Krongthong W, Luengingkasoot S, Sornsamdang G, Patumanond J, Sritipsukho P. Screening values of carcinoembryonic antigen and cytokeratin 19 fragment for lung cancer in combination with low-dose computed tomography in high-risk populations: Initial and 2-year screening outcomes. Lung Cancer. 2018; 122:243–48. https://doi.org/10.1016/j.lungcan.2018.05.012. [PubMed].
6. Wang J, Chu Y, Li J, Wang T, Sun L, Wang P, Fang X, Zeng F, Wang J, Zeng F. The clinical value of carcinoembryonic antigen for tumor metastasis assessment in lung cancer. PeerJ. 2019; 7:e7433. https://doi.org/10.7717/peerj.7433. [PubMed].
7. Chen ZQ, Huang LS, Zhu B. Assessment of Seven Clinical Tumor Markers in Diagnosis of Non-Small-Cell Lung Cancer. Dis Markers. 2018; 2018:9845123. https://doi.org/10.1155/2018/9845123. [PubMed].
8. Cedrés S, Nuñez I, Longo M, Martinez P, Checa E, Torrejón D, Felip E. Serum tumor markers CEA, CYFRA21-1, and CA-125 are associated with worse prognosis in advanced non-small-cell lung cancer (NSCLC). Clin Lung Cancer. 2011; 12:172–79. https://doi.org/10.1016/j.cllc.2011.03.019. [PubMed].
9. Matsuoka K, Sumitomo S, Nakashima N, Nakajima D, Misaki N. Prognostic value of carcinoembryonic antigen and CYFRA21-1 in patients with pathological stage I non-small cell lung cancer. Eur J Cardiothorac Surg. 2007; 32:435–39. https://doi.org/10.1016/j.ejcts.2007.05.014. [PubMed].
10. Tomita M, Matsuzaki Y, Edagawa M, Shimizu T, Hara M, Onitsuka T. Prognostic significance of preoperative serum carcinoembryonic antigen level in lung adenocarcinoma but not squamous cell carcinoma. Ann Thorac Cardiovasc Surg. 2004; 10:76–80. [PubMed].
11. Abbas M, Kassim SA, Habib M, Li X, Shi M, Wang ZC, Hu Y, Zhu HL. Clinical Evaluation of Serum Tumor Markers in Patients With Advanced-Stage Non-Small Cell Lung Cancer Treated With Palliative Chemotherapy in China. Front Oncol. 2020; 10:800. https://doi.org/10.3389/fonc.2020.00800. [PubMed].
12. Grunnet M, Sorensen JB. Carcinoembryonic antigen (CEA) as tumor marker in lung cancer. Lung Cancer. 2012; 76:138–43. https://doi.org/10.1016/j.lungcan.2011.11.012. [PubMed].
13. Lang D, Horner A, Brehm E, Akbari K, Hergan B, Langer K, Asel C, Scala M, Kaiser B, Lamprecht B. Early serum tumor marker dynamics predict progression-free and overall survival in single PD-1/PD-L1 inhibitor treated advanced NSCLC-A retrospective cohort study. Lung Cancer. 2019; 134:59–65. https://doi.org/10.1016/j.lungcan.2019.05.033. [PubMed].
14. Fiala O, Pesek M, Finek J, Benesova L, Minarik M, Bortlicek Z, Topolcan O. Predictive role of CEA and CYFRA 21-1 in patients with advanced-stage NSCLC treated with erlotinib. Anticancer Res. 2014; 34:3205–10. [PubMed].
15. Okada M, Nishio W, Sakamoto T, Uchino K, Yuki T, Nakagawa A, Tsubota N. Prognostic significance of perioperative serum carcinoembryonic antigen in non-small cell lung cancer: analysis of 1,000 consecutive resections for clinical stage I disease. Ann Thorac Surg. 2004; 78:216–21. https://doi.org/10.1016/j.athoracsur.2004.02.009. [PubMed].
16. Kozu Y, Maniwa T, Takahashi S, Isaka M, Ohde Y, Nakajima T. Prognostic significance of postoperative serum carcinoembryonic antigen levels in patients with completely resected pathological-stage I non-small cell lung cancer. J Cardiothorac Surg. 2013; 8:106. https://doi.org/10.1186/1749-8090-8-106. [PubMed].
17. Kobayashi N, Toyooka S, Soh J, Ichimura K, Yanai H, Suehisa H, Ichihara S, Yamane M, Aoe M, Sano Y, Date H. Risk factors for recurrence and unfavorable prognosis in patients with stage I non-small cell lung cancer and a tumor diameter of 20 mm or less. J Thorac Oncol. 2007; 2:808–12. https://doi.org/10.1097/JTO.0b013e31814617c7. [PubMed].
18. Foa P, Fornier M, Miceli R, Seregni E, Santambrogio L, Nosotti M, Cataldo I, Sala M, Caldiera S, Bombardieri E. Tumour markers CEA, NSE, SCC, TPA and CYFRA 21.1 in resectable non-small cell lung cancer. Anticancer Res. 1999; 19:3613–18. [PubMed].
19. Jiao Z, Cao S, Li J, Hu N, Gong Y, Wang L, Jin S. Clinical Associations of Preoperative and Postoperative Serum CEA and Lung Cancer Outcome. Front Mol Biosci. 2021; 8:686313. https://doi.org/10.3389/fmolb.2021.686313. [PubMed].
20. Feng LX, Wang J, Yu Z, Song SA, Zhai WX, Dong SH, Yu HS, Zhang Y. Clinical significance of serum EGFR gene mutation and serum tumor markers in predicting tyrosine kinase inhibitor efficacy in lung adenocarcinoma. Clin Transl Oncol. 2019; 21:1005–13. https://doi.org/10.1007/s12094-018-02014-6. [PubMed].
21. Lang D, Haslinger W, Akbari K, Scala M, Hergan B, Asel C, Horner A, Wass R, Brehm E, Kaiser B, Lamprecht B. Serum Tumor Marker Dynamics as Predictive Biomarkers in NSCLC Chemo-Immunotherapy and Mono-Immunotherapy Maintenance: A Registry-Based Descriptive Study. Lung Cancer (Auckl). 2020; 11:113–21. https://doi.org/10.2147/LCTT.S286228. [PubMed].
22. Clevers MR, Kastelijn EA, Peters BJM, Kelder H, Schramel FMN. Evaluation of Serum Biomarker CEA and Ca-125 as Immunotherapy Response Predictors in Metastatic Non-small Cell Lung Cancer. Anticancer Res. 2021; 41:869–76. https://doi.org/10.21873/anticanres.14839. [PubMed].
23. Zhao T, Mao G, Chen M. The Role of Change Rates of CYFRA21-1 and CEA in Predicting Chemotherapy Efficacy for Non-Small-Cell Lung Cancer. Comput Math Methods Med. 2021; 2021:1951364. https://doi.org/10.1155/2021/1951364. [PubMed]. Retraction in: Comput Math Methods Med. 2023; 2023:9786104. https://doi.org/10.1155/2023/9786104. [PubMed].
24. Zhang Z, Yuan F, Chen R, Li Y, Ma J, Yan X, Wang L, Zhang F, Tao H, Guo D, Huang Z, Zhang S, Li X, et al. Dynamics of Serum Tumor Markers Can Serve as a Prognostic Biomarker for Chinese Advanced Non-small Cell Lung Cancer Patients Treated With Immune Checkpoint Inhibitors. Front Immunol. 2020; 11:1173. https://doi.org/10.3389/fimmu.2020.01173. [PubMed].
25. Liu H, Gu X, Lv T, Wu Y, Xiao Y, Yuan D, Li Y, Song Y. The role of serum carcinoembryonic antigen in predicting responses to chemotherapy and survival in patients with non-small cell lung cancer. J Cancer Res Ther. 2014; 10:239–43. https://doi.org/10.4103/0973-1482.136541. [PubMed].
26. Dal Bello MG, Filiberti RA, Alama A, Orengo AM, Mussap M, Coco S, Vanni I, Boccardo S, Rijavec E, Genova C, Biello F, Barletta G, Rossi G, et al. The role of CEA, CYFRA21-1 and NSE in monitoring tumor response to Nivolumab in advanced non-small cell lung cancer (NSCLC) patients. J Transl Med. 2019; 17:74. https://doi.org/10.1186/s12967-019-1828-0. [PubMed].
27. Zhang N, Kong L, Shi F, Jing W, Wang H, Yang M, Yu J, Zhu H. Kinetic change of serum carcinoembryonic antigen can early predict progression in patients with metastatic non-small cell lung cancer during maintenance therapy with bevacizumab plus pemetrexed. Oncotarget. 2017; 8:74910–16. https://doi.org/10.18632/oncotarget.20456. [PubMed].
28. Arrieta O, Villarreal-Garza C, Martínez-Barrera L, Morales M, Dorantes-Gallareta Y, Peña-Curiel O, Contreras-Reyes S, Macedo-Pérez EO, Alatorre-Alexander J. Usefulness of serum carcinoembryonic antigen (CEA) in evaluating response to chemotherapy in patients with advanced non small-cell lung cancer: a prospective cohort study. BMC Cancer. 2013; 13:254. https://doi.org/10.1186/1471-2407-13-254. [PubMed].
29. Schneider BJ, Ismaila N, Aerts J, Chiles C, Daly ME, Detterbeck FC, Hearn JWD, Katz SI, Leighl NB, Levy B, Meyers B, Murgu S, Nekhlyudov L, et al. Lung Cancer Surveillance After Definitive Curative-Intent Therapy: ASCO Guideline. J Clin Oncol. 2020; 38:753–66. https://doi.org/10.1200/JCO.19.02748. [PubMed].
30. Planchard D, Popat S, Kerr K, Novello S, Smit EF, Faivre-Finn C, Mok TS, Reck M, Van Schil PE, Hellmann MD, Peters S, and ESMO Guidelines Committee. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018; 29:iv192–237. https://doi.org/10.1093/annonc/mdy275. [PubMed].
31. Ettinger DS, Wood DE, Aisner DL, Akerley W, Bauman JR, Bharat A, Bruno DS, Chang JY, Chirieac LR, D’Amico TA, DeCamp M, Dilling TJ, Dowell J, et al. Non-Small Cell Lung Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2022; 20:497–530. https://doi.org/10.6004/jnccn.2022.0025. [PubMed].
32. Ellis PM, Vella ET, Ung YC. The Lung Cancer Disease Site Group. Systemic Treatment for Patients with Advanced Non-Small Cell Lung Cancer. CCO 3(7-10). 2016.
33. Ung YC, Souter LH, Darling G, Dobranowski J, Donohue L, Leighl N, Ellis PM. Lung Cancer Follow-up Expert Panel. Follow-up and Surveillance of Curatively Treated Lung Cancer Patients. CCO (26-3). 2014.
34. Kris MG, Gaspar LE, Chaft JE, Kennedy EB, Azzoli CG, Ellis PM, Lin SH, Pass HI, Seth R, Shepherd FA, Spigel DR, Strawn JR, Ung YC, Weyant M. Adjuvant Systemic Therapy and Adjuvant Radiation Therapy for Stage I to IIIA Completely Resected Non-Small-Cell Lung Cancers: American Society of Clinical Oncology/Cancer Care Ontario Clinical Practice Guideline Update. J Clin Oncol. 2017; 35:2960–74. https://doi.org/10.1200/JCO.2017.72.4401. [PubMed].
35. Molina R, Filella X, Augé JM, Fuentes R, Bover I, Rifa J, Moreno V, Canals E, Viñolas N, Marquez A, Barreiro E, Borras J, Viladiu P. Tumor markers (CEA, CA 125, CYFRA 21-1, SCC and NSE) in patients with non-small cell lung cancer as an aid in histological diagnosis and prognosis. Comparison with the main clinical and pathological prognostic factors. Tumour Biol. 2003; 24:209–18. https://doi.org/10.1159/000074432. [PubMed].
36. Holdenrieder S, Wehnl B, Hettwer K, Simon K, Uhlig S, Dayyani F. Carcinoembryonic antigen and cytokeratin-19 fragments for assessment of therapy response in non-small cell lung cancer: a systematic review and meta-analysis. Br J Cancer. 2017; 116:1037–45. https://doi.org/10.1038/bjc.2017.45. [PubMed].
37. Yang L, Chen X, Li Y, Yang J, Tang L. Declines in serum CYFRA21-1 and carcinoembryonic antigen as predictors of chemotherapy response and survival in patients with advanced non-small cell lung cancer. Exp Ther Med. 2012; 4:243–48. https://doi.org/10.3892/etm.2012.570. [PubMed].
38. Ardizzoni A, Cafferata MA, Tiseo M, Filiberti R, Marroni P, Grossi F, Paganuzzi M. Decline in serum carcinoembryonic antigen and cytokeratin 19 fragment during chemotherapy predicts objective response and survival in patients with advanced nonsmall cell lung cancer. Cancer. 2006; 107:2842–49. https://doi.org/10.1002/cncr.22330. [PubMed].
39. Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O’Neal L, McLeod L, Delacqua G, Delacqua F, Kirby J, Duda SN, and REDCap Consortium. The REDCap consortium: Building an international community of software platform partners. J Biomed Inform. 2019; 95:103208. https://doi.org/10.1016/j.jbi.2019.103208. [PubMed].
40. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S, Mooney M, Rubinstein L, Shankar L, Dodd L, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009; 45:228–47. https://doi.org/10.1016/j.ejca.2008.10.026. [PubMed].
41. Seymour L, Bogaerts J, Perrone A, Ford R, Schwartz LH, Mandrekar S, Lin NU, Litière S, Dancey J, Chen A, Hodi FS, Therasse P, Hoekstra OS, et al, and RECIST working group. iRECIST: guidelines for response criteria for use in trials testing immunotherapeutics. Lancet Oncol. 2017; 18:e143–52. https://doi.org/10.1016/S1470-2045(17)30074-8. [PubMed].