
Introduction
Cancer-associated malnutrition is a common and significant clinical issue because it is often unrecognized and undertreated. Gastric cancer patients are often malnourished at the time of diagnosis, which is related to impaired digestion, malabsorption, and bleeding and/or protein loss from the primary lesion [1, 2]. Recent studies have indicated that the preoperative nutritional and immunological statuses are not only associated with postoperative complications but also with long-term prognosis among cancer patients [3–5]. Moreover, several studies have demonstrated that postoperative complications adversely affect long-term survival [6–8]. Therefore, the preoperative assessment of nutritional status and preoperative nutritional management may help improve short-term outcome and long-term prognosis in gastric cancer patients who undergoing laparoscopic gastrectomy.
The prognostic nutrition index (PNI), which predicts the risk of postoperative complications, is calculated using serum albumin level and total number of lymphocytes [9]. Serum albumin has been reported to reflect nutrition and the immune response, being indicative of macrophage activation, tumor progression, and prognosis [10, 11]. Lymphocytes have been found to activate the adaptive immune system to stop cancer dispersion [12, 13]. Albumin level and lymphocyte count balance is closely linked to immune and nutritional status and is reported to affect the prognosis of cancer patients [10–13]. In addition, basic nutrition and systemic inflammation are also reported to be associated with the long-term prognosis of cancer patients [14–16]. However, the clinical significance of PNI in patients with gastric cancer remains controversial. Therefore, this study aimed to evaluate the relationship between preoperative nutrition and immunological status (using PNI) and short-term outcome and long-term prognosis, especially among stage-stratified gastric cancer patients undergoing curative gastrectomy.
Results
Background characteristics and PNI
Based on a PNI cut-off of 44.2, 118 (27.2%) and 316 (72.8%), patients were classified into the low and high PNI groups, respectively. Significant differences were observed in age, body mass index (BMI), tumor diameter, tumor stage, pathological TNM (pTNM) stage, surgical procedure, intraoperative blood loss, and C-reactive protein (CRP) level (Table 1).
Table 1: Relationships between PNI and clinicopathological features
| Characteristics | No. of Patients | PNI | p value | |
|---|---|---|---|---|
| <44.2 (n = 118) | ≥44.2 (n = 316) | |||
| Age (years) | 77 (46–91) | 69 (36–89) | <0.001 | |
| Sex | 0.885 | |||
| Male | 303 | 83 | 220 | |
| Female | 131 | 35 | 96 | |
| BMI | 21.3 (14.0–30.5) | 22.6 (16.5–40.4) | <0.001 | |
| Tumor location | 0.315 | |||
| EGJ | 11 | 2 | 9 | |
| U | 85 | 28 | 57 | |
| M | 184 | 43 | 141 | |
| L | 154 | 45 | 109 | |
| Tumor size (mm) | 55 (7–170) | 38 (3–180) | <0.001 | |
| Histological differentiation | 0.151 | |||
| Well | 81 | 15 | 66 | |
| Moderate | 162 | 47 | 115 | |
| Poor | 191 | 56 | 135 | |
| Depth of tumor | <0.001 | |||
| T1a–1b | 232 | 45 | 187 | |
| 2 | 56 | 14 | 42 | |
| 3 | 58 | 19 | 39 | |
| 4a–4b | 88 | 40 | 48 | |
| Lymph node metastasis | 0.072 | |||
| N0 | 284 | 66 | 218 | |
| N1 | 48 | 15 | 33 | |
| N2 | 53 | 20 | 33 | |
| N3 | 49 | 17 | 32 | |
| pTNM stage | <0.001 | |||
| 1a–1b | 260 | 52 | 208 | |
| 2a–2b | 69 | 24 | 45 | |
| 3a–3c | 105 | 42 | 63 | |
| Operative procedure | 0.047 | |||
| Total | 91 | 34 | 57 | |
| Proximal | 44 | 10 | 34 | |
| Distal | 299 | 74 | 225 | |
| Operation time (min) | 394 (177–911) | 384 (70–881) | 0.825 | |
| Intraoperative blood loss | 57.5 (0–2620) | 30 (0–4070) | 0.007 | |
| Postoperative complications | 0.146 | |||
| Present | 128 | 41 | 87 | |
| Absent | 306 | 77 | 229 | |
| CRP (mg/dl) | 0.20 (0.01–11.10) | 0.06 (0.002–6.31) | <0.001 | |
| CEA (ng/ml) | 3.6 (0.8–163.3) | 3.2 (0.7–161.1) | 0.089 | |
| Adjuvant chemotherapy | 0.143 | |||
| Yes | 124 | 38 | 86 | |
| No | 310 | 80 | 230 | |
Background characteristics and postoperative complications
Among the 434 patients, 128 (29.4%) experienced postoperative complications (Table 2). Significant differences were observed in age, sex, tumor location, surgical procedure, operation time, and serum CRP level. The postoperative complications were not associated with PNI.
Table 2: Relationships between postoperative complications and clinicopathological features
| Characteristics | No. of Patients | Postoperative complications | p value | |
|---|---|---|---|---|
| Absent (n = 306) | Present (n = 128) | |||
| Age (years) | 77 (46–91) | 69 (36–89) | <0.001 | |
| Sex | 0.025 | |||
| Male | 303 | 204 | 99 | |
| Female | 131 | 102 | 29 | |
| BMI | 22.2 (14.7–40.4) | 22.3 (14.0–32.5) | 0.354 | |
| Tumor location | <0.001 | |||
| EGJ | 11 | 5 | 6 | |
| U | 85 | 43 | 42 | |
| M | 184 | 142 | 42 | |
| L | 154 | 116 | 38 | |
| Tumor size (mm) | 40 (3–176) | 40 (3–180) | 0.654 | |
| Histological differentiation | 0.851 | |||
| Well | 81 | 55 | 26 | |
| Moderate | 162 | 115 | 47 | |
| Poor | 191 | 136 | 55 | |
| Depth of tumor | 0.334 | |||
| T1a-1b | 232 | 172 | 60 | |
| 2 | 56 | 38 | 18 | |
| 3 | 58 | 37 | 21 | |
| 4a-4b | 88 | 59 | 29 | |
| Lymph node metastasis | 0.337 | |||
| N0 | 284 | 205 | 79 | |
| N1 | 48 | 35 | 13 | |
| N2 | 53 | 37 | 16 | |
| N3 | 49 | 29 | 20 | |
| pTNM stage | 0.190 | |||
| 1a-1b | 260 | 191 | 69 | |
| 2a-2b | 69 | 48 | 21 | |
| 3a-3c | 105 | 67 | 38 | |
| Operative procedure | <0.001 | |||
| Total | 91 | 49 | 42 | |
| Proximal | 44 | 22 | 22 | |
| Distal | 299 | 235 | 64 | |
| Operation time (min) | 379 (70–911) | 413 (207–836) | 0.009 | |
| Intraoperative blood loss | 40 (0–4070) | 50 (0–1580) | 0.200 | |
| CRP (mg/dl) | 0.07 (0.01–6.31) | 0.10 (0.002–11.10) | 0.006 | |
| CEA (ng/ml) | 3.2 (0.7–106.0) | 3.4 (0.7–163.3) | 0.199 | |
| PNI | 0.146 | |||
| ≥44.2 | 316 | 229 | 87 | |
| <44.2 | 118 | 77 | 41 | |
| Adjuvant chemotherapy | 0.894 | |||
| Yes | 124 | 88 | 36 | |
| No | 310 | 218 | 92 | |
Impact of PNI on OS among all patients
Univariate analysis of risk factors for OS age, BMI, tumor diameter, tumor differentiation, pTNM stage, carcinoembryonic antigen (CEA), CRP level, PNI, postoperative complications, and postoperative adjuvant chemotherapy were significant relevant factors. In multivariate analyses, pTNM stage (p < 0.001), CEA (p = 0.003), and PNI (p < 0.001) were found to be independent predictive factors for OS (Table 3).
Table 3: Univariate and multivariate analyses of clinicopathological factors for overall survival
| Variables | Category or characteristics | Patients (n = 368) | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p value | HR | 95% CI | p value | |||
| Age | (<70/≥70) | 166/202 | 1.617 | 1.043–2.505 | 0.032 | 1.068 | 0.659–1.731 | 0.790 |
| Sex | (Female/Male) | 114/254 | 1.604 | 0.974–2.642 | 0.063 | |||
| BMI | (≥18.5/<18.5) | 332/36 | 1.905 | 1.075–3.375 | 0.027 | 1.396 | 0.740–2.634 | 0.304 |
| Tumor size | (<5/≥5) | 217/151 | 2.334 | 1.525–3.573 | <0.001 | 0.912 | 0.523–1.589 | 0.745 |
| Histological differentiation | (well & mod/poor) | 163/205 | 1.656 | 1.087–2.522 | 0.019 | 1.473 | 0.930–2.331 | 0.099 |
| pTNM stage | (1, 2/3) | 282/86 | 4.000 | 2.612–6.125 | <0.001 | 3.047 | 1.687–5.505 | <0.001 |
| CEA | (<5.0/≥5.0) | 286/82 | 2.350 | 1.528–3.612 | <0.001 | 1.975 | 1.255–3.107 | 0.003 |
| CRP | (≦0.5/>0.5) | 312/56 | 2.674 | 1.691–4.229 | <0.001 | 1.249 | 0.709–2.201 | 0.441 |
| PNI | (≥44.2/<44.2) | 254/114 | 3.750 | 2.463–5.711 | <0.001 | 2.808 | 1.701–4.637 | <0.001 |
| Postoperative Complications | (Absent/Present) | 265/103 | 1.876 | 1.220–2.884 | 0.004 | 1.427 | 0.884–2.305 | 0.146 |
| Adjuvant chemotherapy | (no/yes) | 268/100 | 1.960 | 1.284–2.990 | 0.002 | 0.995 | 0.580–1.706 | 0.986 |
OS stratified according to PNI
The OS curve for the low PNI group was significantly inferior to that of the high PNI group; this was reflected in the significantly lower OS rate at five-years after surgery (51.1% vs. 91.2%, respectively; p < 0.001) (Figure 1).
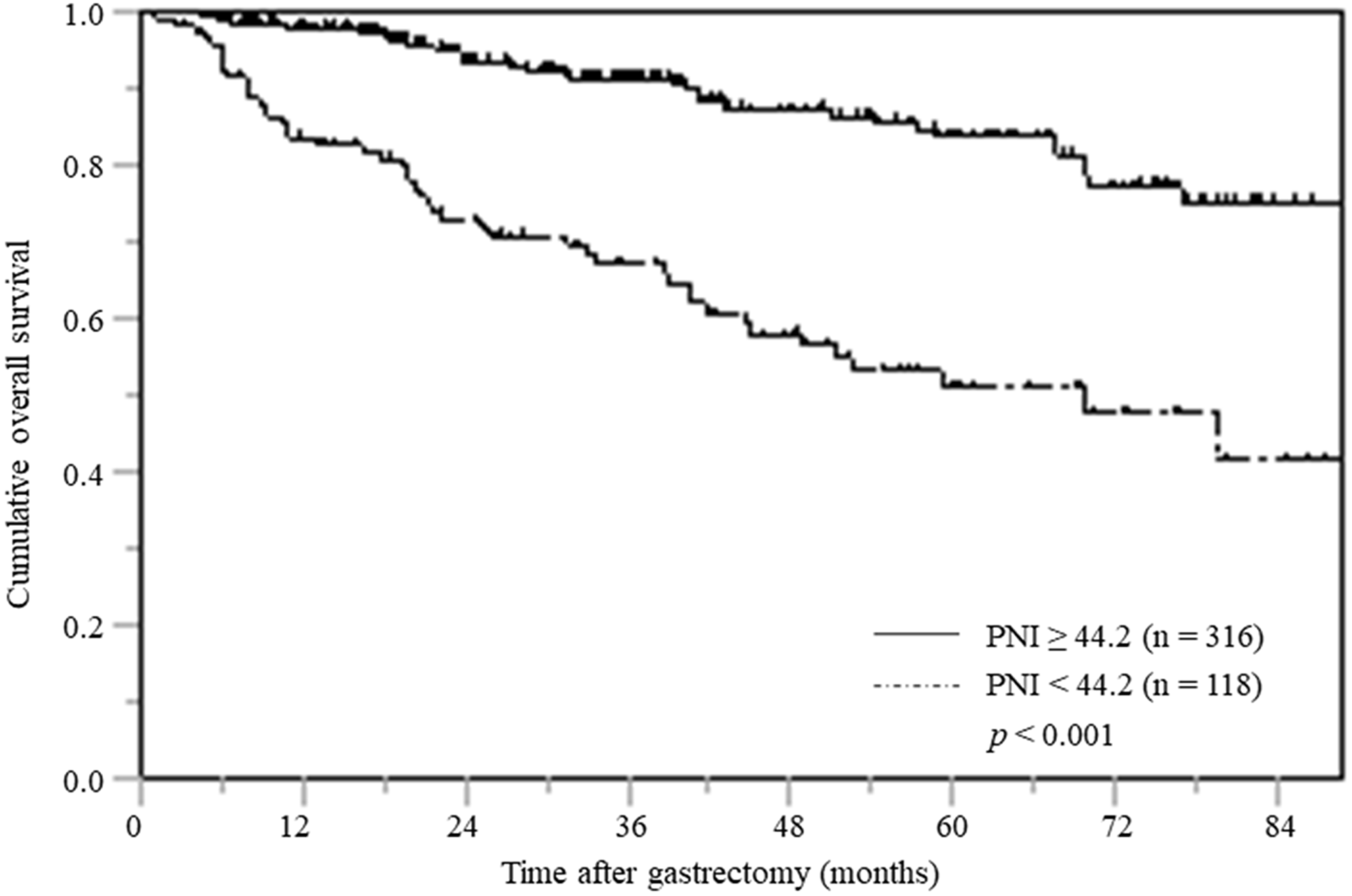
Figure 1: Overall survival based on PNI.
Impact on postoperative complications
Univariate analysis of risk factors for postoperative complications showed that sex, CRP level, PNI, and surgical procedures were significant relevant factors. Multivariate analyses showed that PNI (p = 0.031) and surgical procedure (p = 0.011) were independent risk factors (Table 4).
Table 4: Univariate and multivariate analyses to assess the risk factors for postoperative complications
| Variables | Category or characteristics | Patients (n = 368) | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p value | OR | 95% CI | p value | |||
| Age | (<70/≥70) | 166/202 | 1.452 | 0.955–2.207 | 0.081 | |||
| Sex | (Female/Male) | 114/254 | 1.707 | 1.059–2.751 | 0.028 | 1.464 | 0.879–2.442 | 0.143 |
| BMI | (≥18.5/<18.5) | 332/ 36 | 0.933 | 0.450–1.937 | 0.853 | |||
| Tumor size | (<5/≥5) | 217/151 | 0.972 | 0.638–1.481 | 0.895 | |||
| Histological differentiation | (well & mod/poor) | 163/205 | 0.972 | 0.642–1.473 | 0.894 | |||
| pTNM stage | (1,2/3) | 282/86 | 1.631 | 0.996–2.672 | 0.052 | |||
| CEA | (<5.0/≥5.0) | 286/82 | 1.369 | 0.851–2.200 | 0.195 | |||
| CRP | (≦0.5/>0.5) | 312/56 | 2.370 | 1.382–4.066 | 0.002 | 1.716 | 0.907–3.249 | 0.097 |
| PNI | (≥44.2/<44.2) | 254/114 | 6.228 | 2.147–18.066 | <0.001 | 4.003 | 1.132–14.153 | 0.031 |
| Operative Procedure | (proximal & distal/total) | 286/82 | 2.300 | 1.389 – 3.806 | 0.001 | 1.968 | 1.167–3.319 | 0.011 |
| Adjuvant chemotherapy | (no/yes) | 268/100 | 0.969 | 0.613–1.532 | 0.894 | |||
Impact of postoperative complications on OS
The OS of the patients with postoperative complications was 74.2% and 65.2% at three-year and five-year, respectively. The OS of the patients without postoperative complications was 88.5% and 77.7% at three-year and five-year, respectively. The OS curve for the patients with postoperative complications was significantly inferior to that of the patients without complications (p = 0.004) (Figure 2).
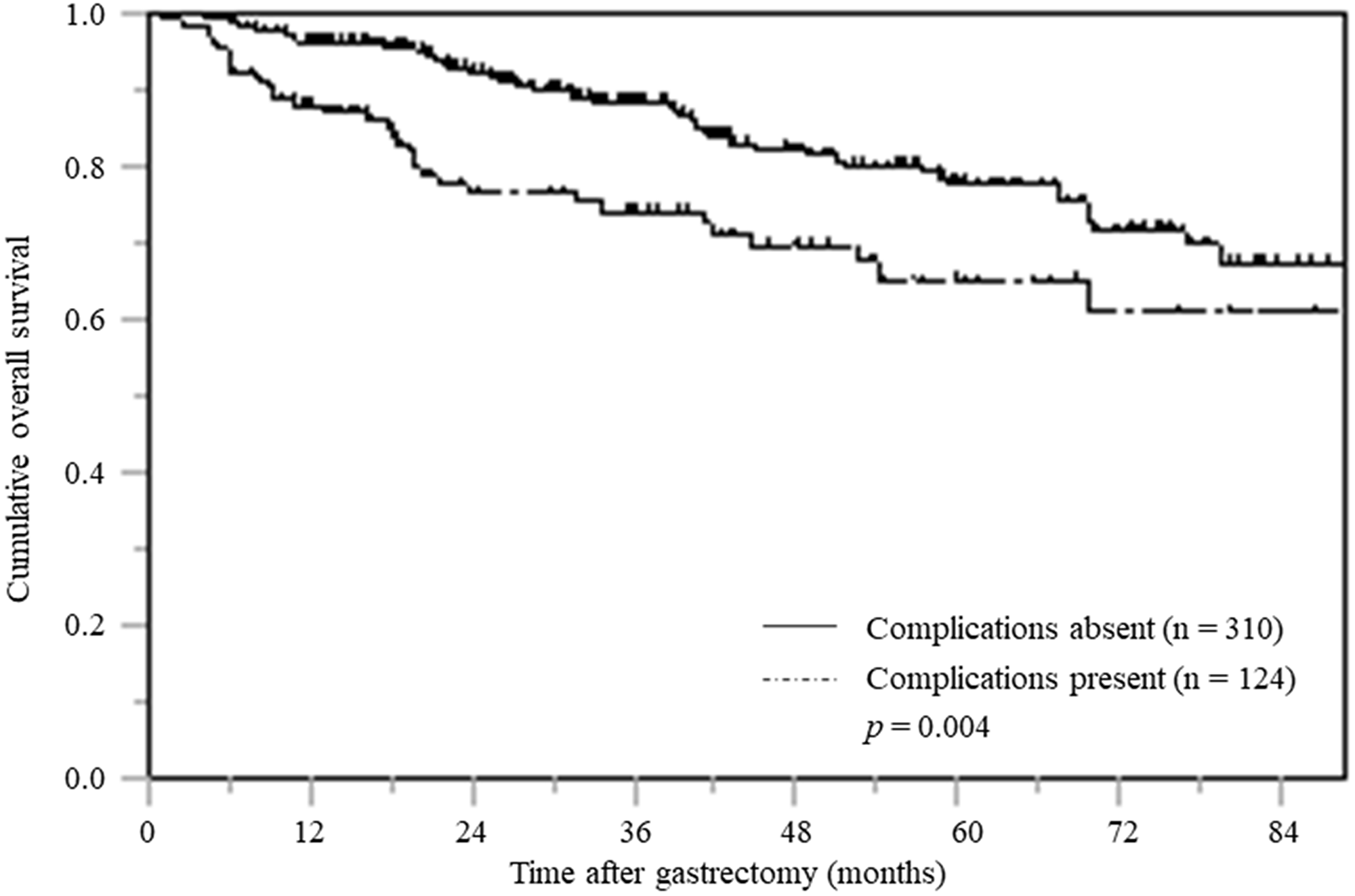
Figure 2: Overall survival based on postoperative complications (CD≧II).
OS and complications stratified by PNI
Among the 118 patients with low PNI, the three-year and five-year OS in the patients with postoperative complications was 50.8% and 37.8%, respectively; while the three-year and five-year OS in the patients without complications was 76.2% and 58.4%, respectively. Among patients with low PNI, those with postoperative complications had significantly inferior OS than those without postoperative complications (p = 0.007) (Figure 3A).
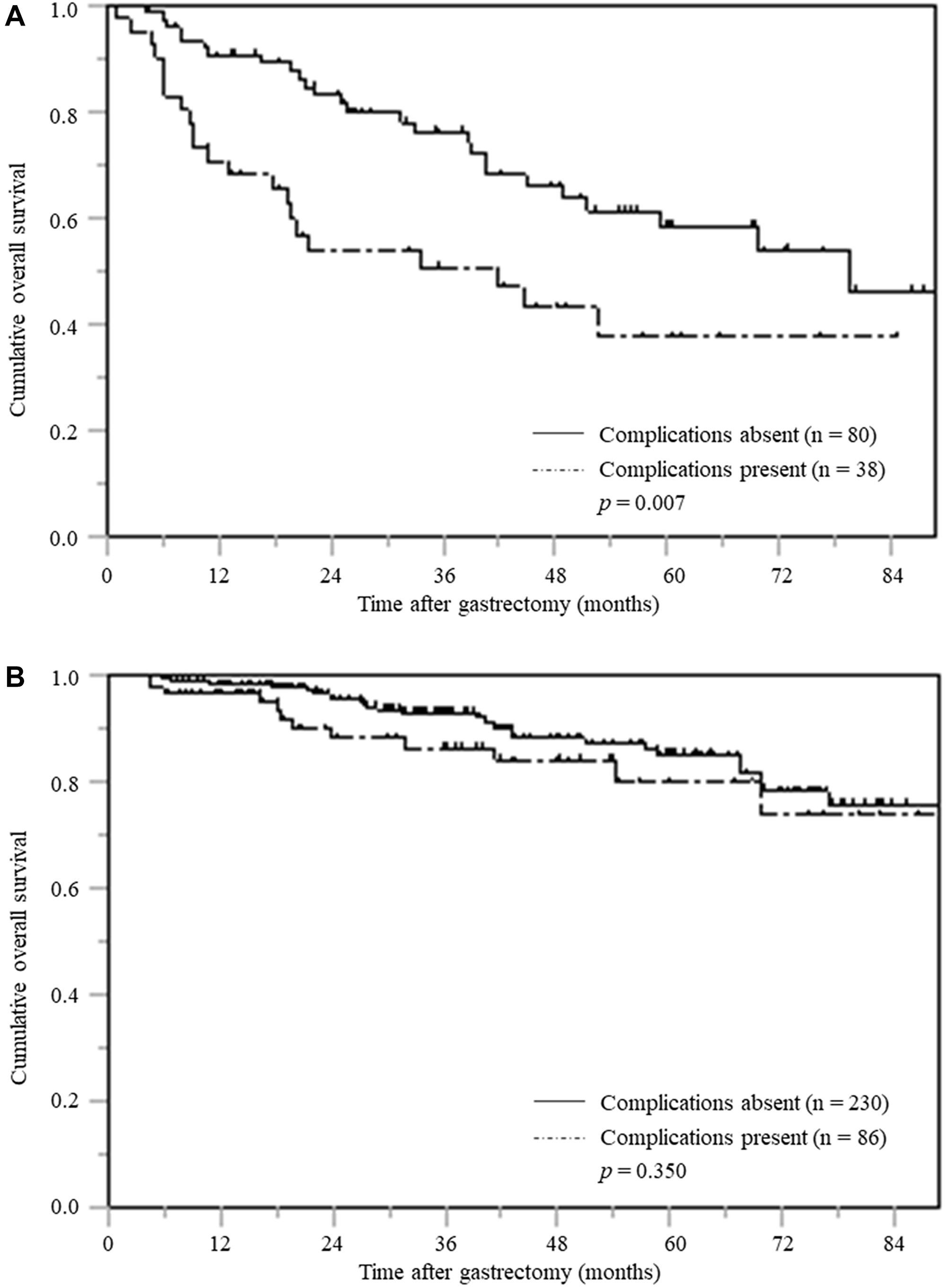
Figure 3: Overall survival based on postoperative complications stratified according to PNI. (A) Low PNI (B) High PNI.
However, in 316 patients with high PNI, there was no significant difference in OS between those with and without postoperative complications. (p = 0.350) (Figure 3B).
OS based on postoperative complications stratified by pTNM stage
Of the 260 patients with pTNM stage I, the OS curve for the patients with postoperative complications was significantly inferior to that of the patients without postoperative complications (p = 0.029) (Figure 4A).
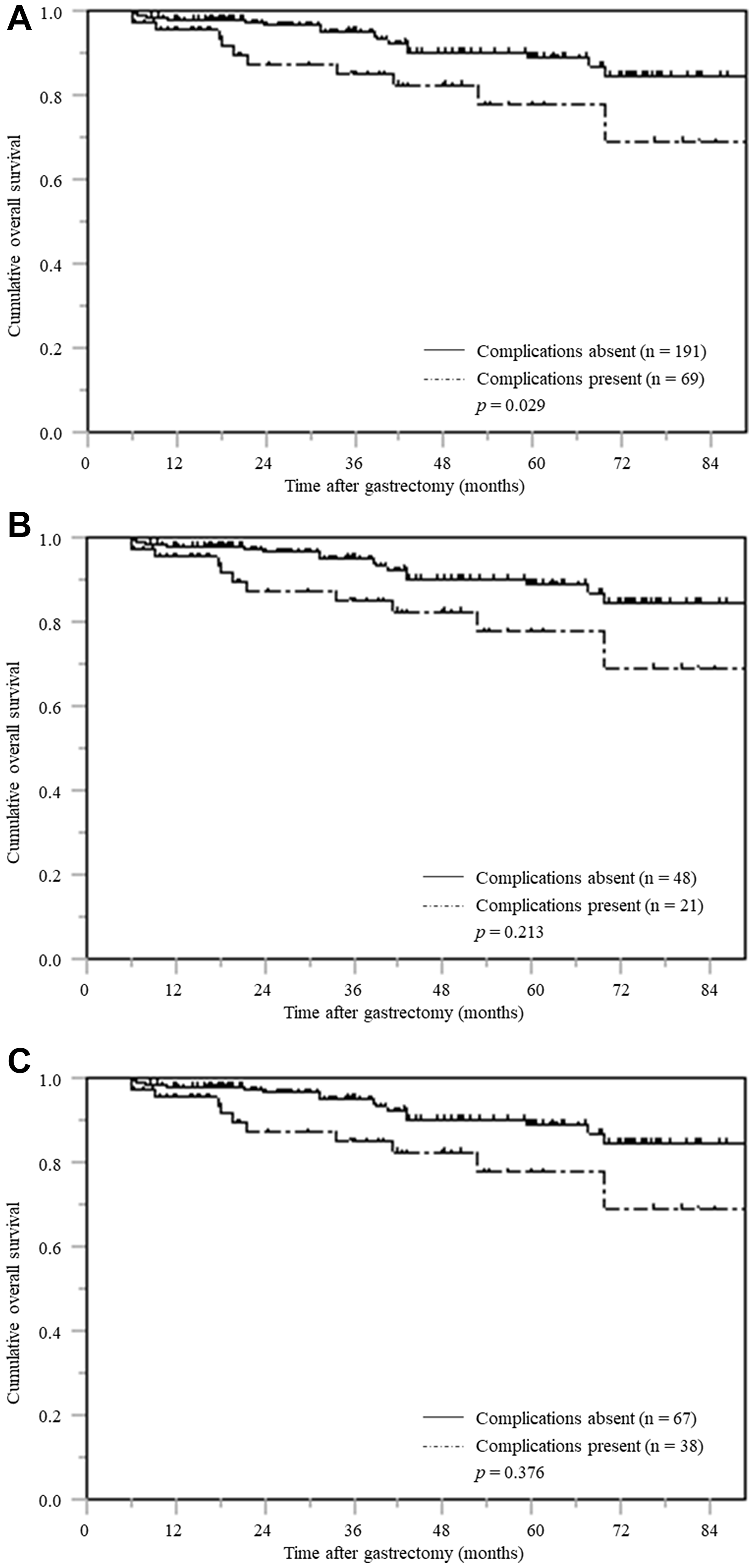
Figure 4: Overall survival based on postoperative complications stratified according by pTNM stage (A) pTNM stage I (B) pTNM stage II (C) pTNM stage III.
However, among patients with pTNM stages II and III, the OS of those with and without postoperative complications did not differ significantly (Figure 4B and 4C).
OS based on postoperative complications stratified by PNI for each pTNM stage
Among patients pTNM stage I patients with low PNI, the OS curve for the patients with postoperative complications was significantly inferior to that of the patients without postoperative complications (p = 0.028) (Figure 5A). However, among high PNI patients, there was no significant difference in OS among those with and without postoperative complications (Figure 5B). Similarly, among pTNM stage II patients with low PNI, those with complications had significantly inferior OS than those without postoperative complications (p = 0.029) (Figure 6A). However, there was no significant difference in OS between patients with and without postoperative complications in high PNI group (p = 0.667) (Figure 6B).
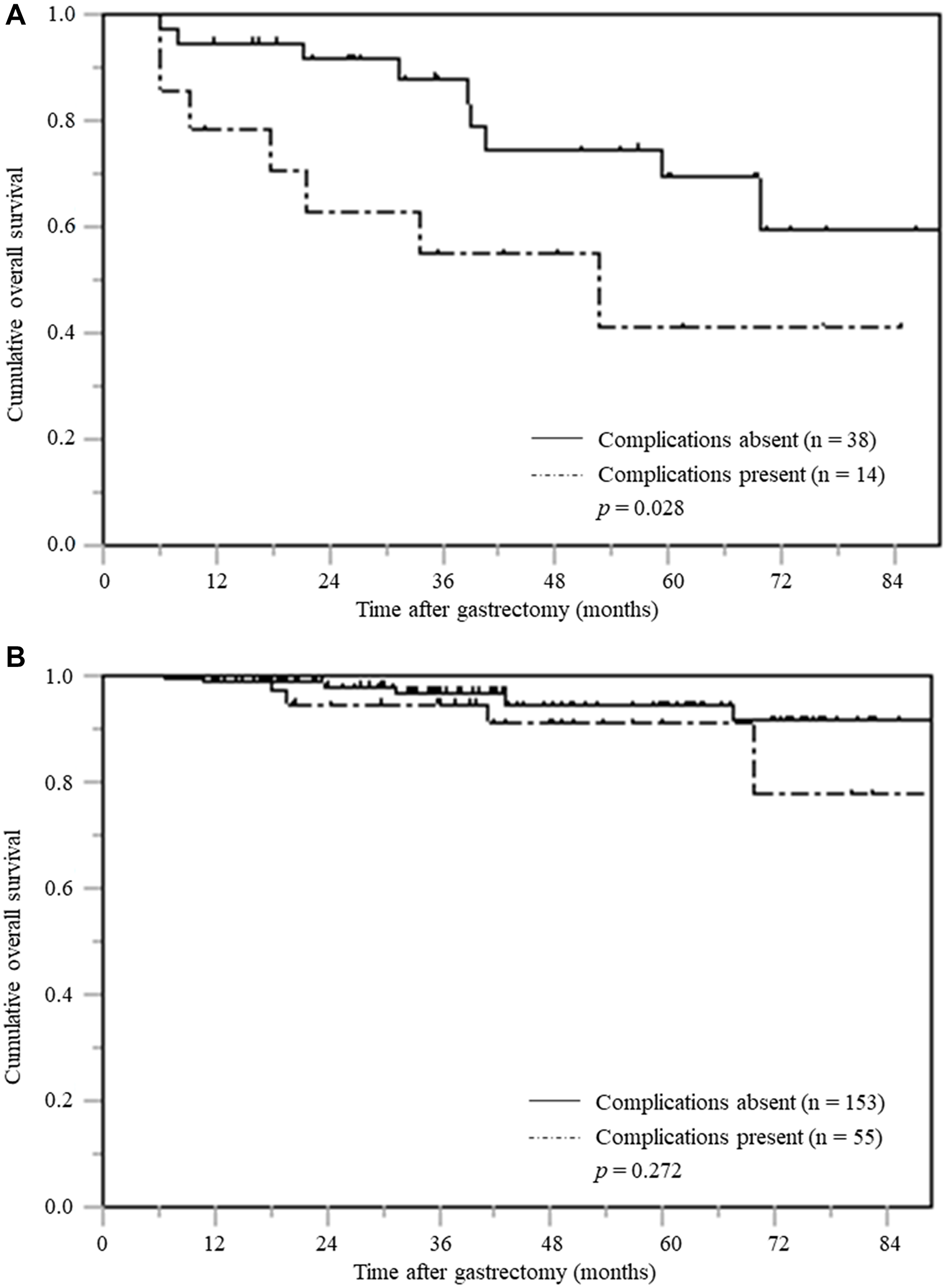
Figure 5: Overall survival based on postoperative complications stratified by PNI in patients with pTNM stage I. (A) Low PNI (B) High PNI.
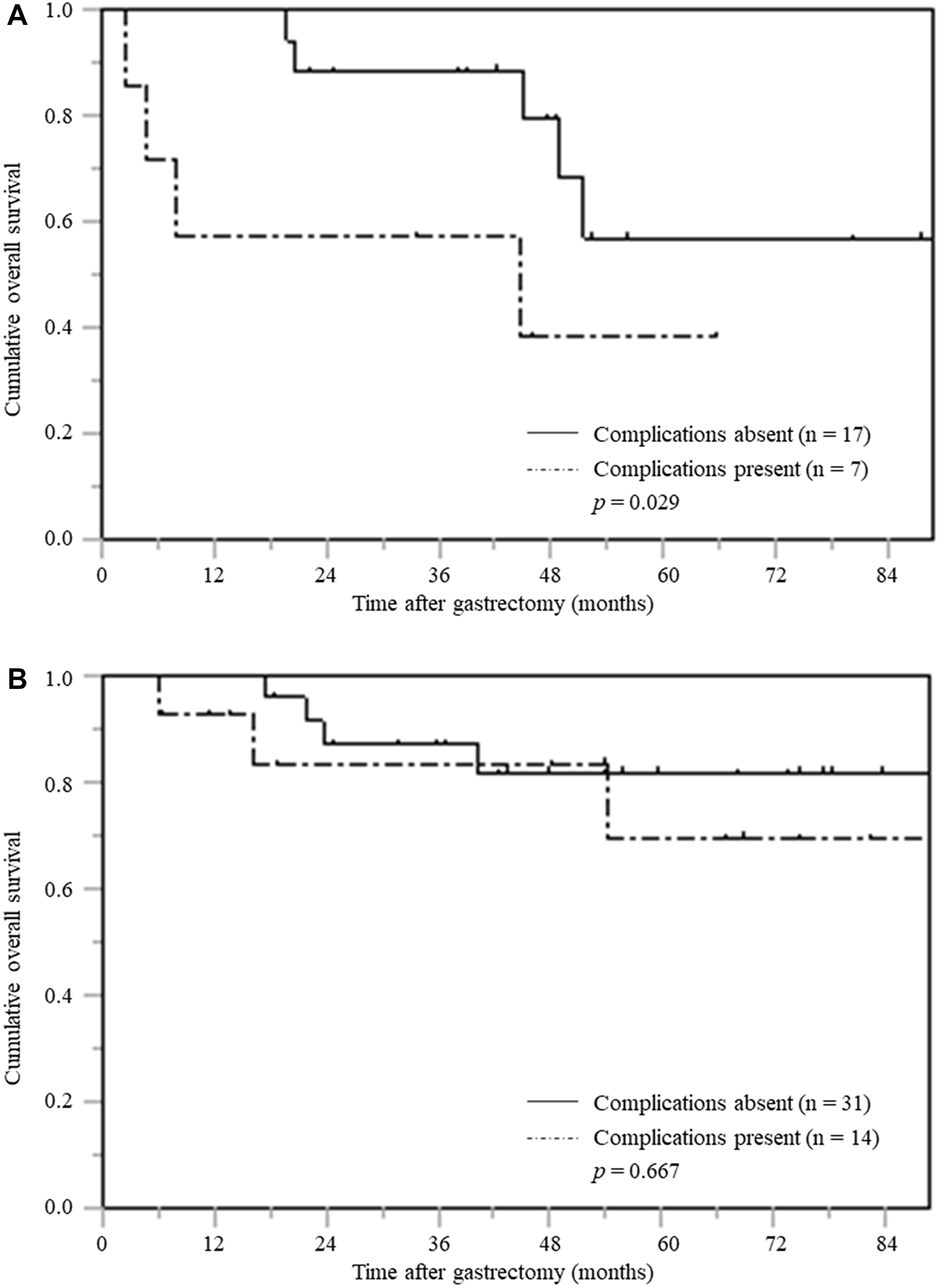
Figure 6: Overall survival based on postoperative complications stratified by PNI in patients with pTNM stage II. (A) Low PNI (B) High PNI.
Meanwhile, among pTNM stage III patients, there was no significant difference in OS between those with and without postoperative complications when stratified according to PNI value (Figure 7A and 7B).
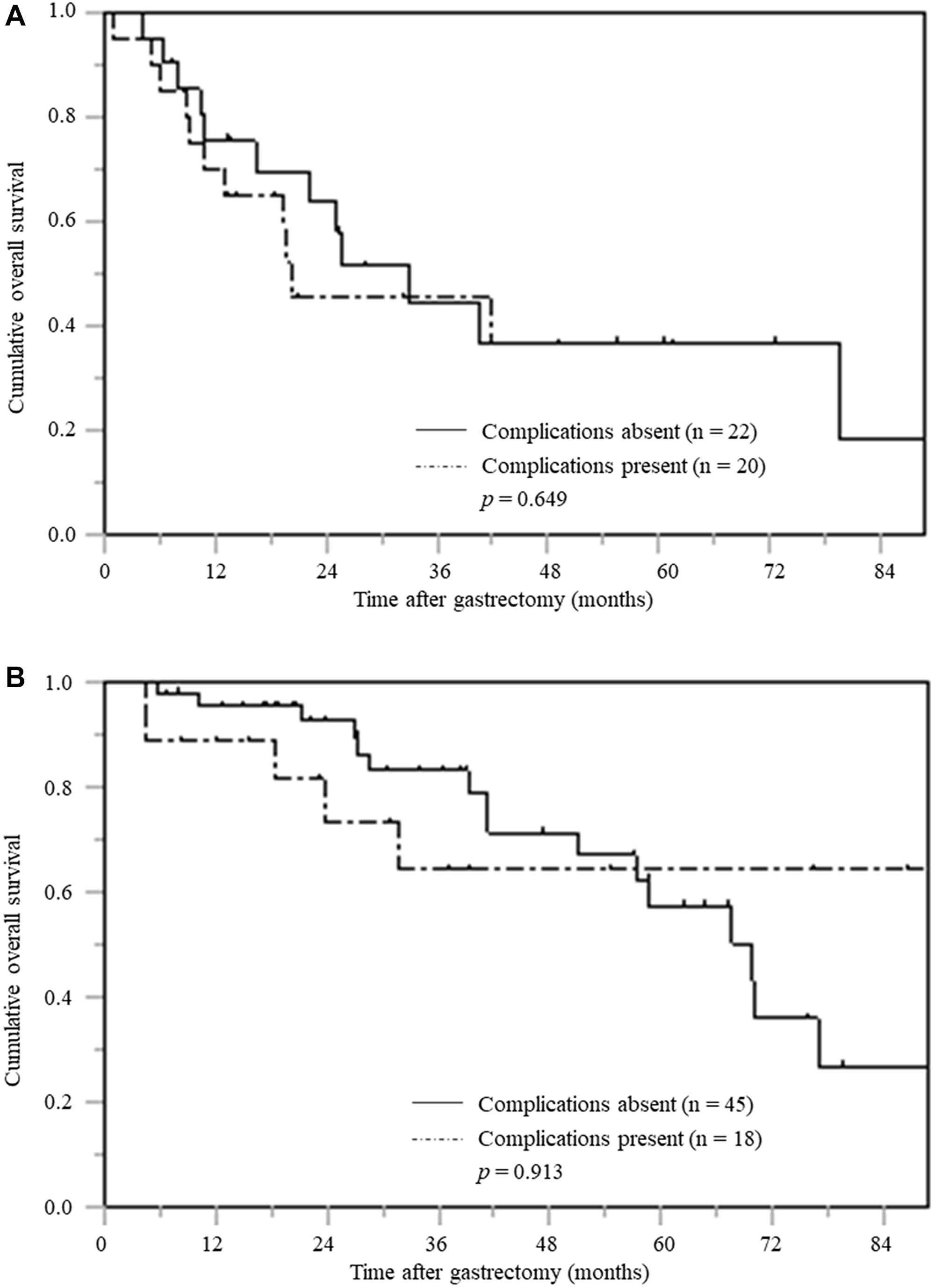
Figure 7: Overall survival based on postoperative complications stratified by PNI in patients with pTNM stage III. (A) Low PNI (B) High PNI.
DISCUSSION
Recent studies have shown that postoperative complications such as anastomotic leakage and postoperative infections adversely affect the prognosis of gastric cancer patients [3, 17–20]. Similarly, in this study we confirmed that presence of postoperative complications significantly predicted worse prognosis, and the type of surgical procedure and PNI were independent risk factors for postoperative complications. Interestingly, long-term prognosis was found to unaffected by postoperative complications among well-nourished gastric cancer patients (i.e., patients with a high preoperative PNI). Although the degree of immunosuppression was not assessed in this study, we consider that postoperative complications increased surgical stress due to local and systemic inflammatory responses, resulting in more severe immunosuppression in the low PNI group than in the high PNI group [21, 22]. Therefore, well-nourished patients may be able to tolerate immunosuppression associated with inflammatory cytokines induced by postoperative complications [3, 23, 24]. Accordingly, we speculated that PNI can be a comprehensive indicator of nutrition and immunological status in gastric cancer patient. Preoperative nutritional interventions, based on preoperative PNI assessments, can reduce the postoperative complication and lead to improvement in therapeutic effect and long-term prognosis. However, because of the limited time between cancer identification and therapeutic surgery, preoperative malnutrition cannot be improved substantially in a short term for advanced cancer [25, 26]. The results of several studies have been inconsistent regarding the efficacy of preoperative nutritional intervention, and it may be difficult to introduce preoperative nutritional interventions to improve OS.
In the stage-stratified analysis, pTNM stage I patients who developed postoperative complications had a significantly inferior prognosis than those without complications, whereas there was no difference in prognosis with respect to postoperative complications in stage II and III patients. In addition, among stage I and II gastric cancer patients, those with low PNI who developed postoperative complications had a significantly inferior OS compared to those without postoperative complications, whereas there was no difference in high PNI patients. And among pTNM stage III patients, there was no significant difference in OS between those with and without complications, regardless of PNI value. These findings suggest that preoperative nutritional status, similar to postoperative complications, is crucial in the prognosis of gastric cancer, especially in relatively early-stage cancer, whereas the association of degree of cancer stage outweighs that of postoperative complications with OS in advanced-stage cancer [27, 28].
In clinical practice, TNM staging alone cannot be used to predict clinical outcomes, since it only classifies patients according to postoperative pathological outcomes and does not include nutritional or inflammatory status [29, 30]. Thus, novel relevant prognostic predictors are needed to improve prognosis with individual treatment for gastric cancer. Recently, researchers have focused not only on tumor itself, but also on the tumor’s microenvironment, especially the immunonutrition and inflammatory status [31–33]. This study showed that PNI is important in assessing the risk of postoperative complications and is an independent predictor of long-term prognosis in gastric cancer patients. Considering the fact, we believe that PNI can effectively complement TNM staging and provide valuable information for individualized prognosis of gastric cancer patients.
While the current study has some advantages over previous reports, it has some potential limitations and caution should be exercised when interpreting the results. First, this was a single-institutional study with a relatively small number of patients and a relatively short follow-up period for evaluation of long-term prognosis. The follow-up period was sufficient to assess the outcome of postoperative complications, but further research is needed to investigate the impact of PNI on long-term prognosis. Second, immunonutritional parameters and systemic levels of inflammatory cytokines were not assessed. Third, the subgroup-derived evidence did not have sufficient statistical power to validate various conclusions because of the small number of patients. Fourth, the analysis did not include factors that could affect inflammation and nutritional markers, such as medication and comorbidity. Fifth, OS was evaluated in this study as it is considered the gold standard endpoint in cancer prognosis studies. However, disease-specific survival and recurrence-free survival data analysis would also provide to be useful. They were not analyzed.
In conclusion, this study suggested that PNI is useful in identifying gastric cancer patients who would benefit from preoperative nutritional management and have an improved prognosis. However, it is unclear whether PNI serve as a nutritional parameter for selecting candidates for nutritional management. Future prospective studies are needed to determine whether aggressive preoperative nutritional management can increase preoperative PNI and improve short-term outcomes and long-term prognosis.
Materials and Methods
Patients
We retrospectively investigated the medical records of 434 gastric cancer patients who undergoing curative laparoscopic gastrectomy between 2010 and 2018. The gastrectomy and lymphadenectomy were determined by the Japanese Gastric Cancer Treatment Guidelines (version 4) [34]. The pathological classification was judged based on the International Union Against Cancer (UICC) TNM 7th edition [35]. The ethics committee of Shimane university approved this study.
Outcomes
Postoperative complications of grade II or higher according to the Clavien-Dindo (CD) classification were retrospectively determined from the patients’ records [36]. Postoperative complications associated with gastric resection were defined as bleeding, anastomotic leakage and stenosis, pancreatic fistula, ascites, surgical site infection, abscess, pleural effusion, deep vein thrombosis/ pulmonary embolism, intestinal paralysis and any organ disease or infection. OS was calculated from the date of gastrectomy to the date of death due to any cause or the last follow-up.
Preoperative nutritional parameters
PNI and BMI, were calculated using laboratory data obtained within 1 week preoperatively. PNI was proposed by Onodera et al. [9].
The receiver operating characteristics (ROC) curve and area under curve (AUC) analyses were performed to determine the optimal cut-off value of PNI for OS. Based on this analysis, cut-off value of PNI was set at 44.2 (sensitivity, 55.7%; specificity, 79.8%; AUC = 0.701) (Figure 8).
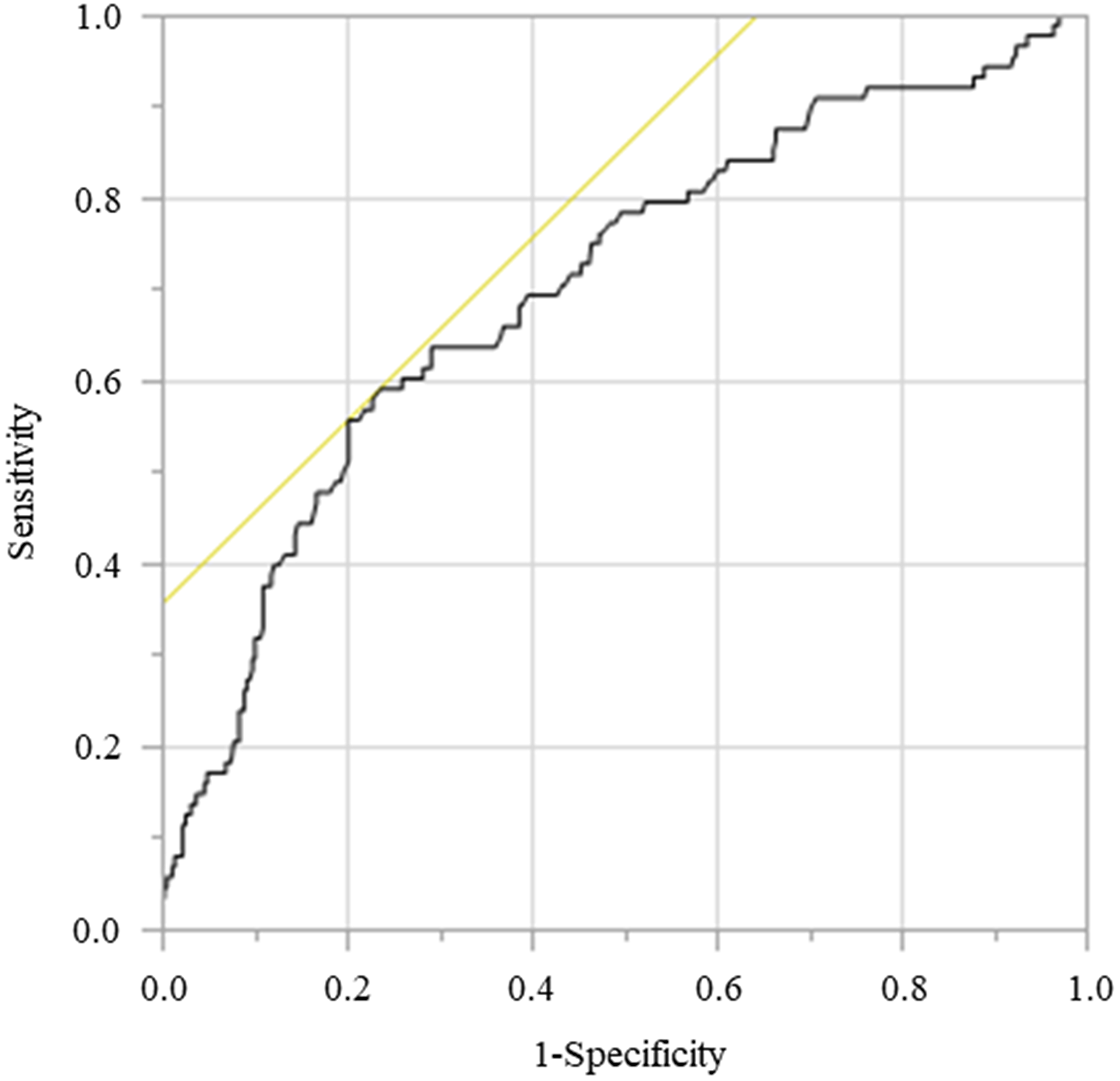
Figure 8: Receiver operating curve for OS was plotted to verify the optimum cut-off value of PNI.
Statistical analyses
Continuous variables are represented as median and range. Differences between groups were assessed using Student’s t-test. Differences between categorical variables were analyzed using the chi-square test. The OS was analyzed using the Kaplan-Meier method and the Log-rank test. In addition, a univariate analysis was performed to identify significantly relevant variables, and variables with a univariate p-value <0.05 were included in the subsequent multivariate analysis. The Cox proportional hazards model used HR and a 95% confidence interval (95% CI). Statistical analysis was performed using JMP software (version 16, USA), and p < 0.05 was judged to be a statistically significant difference.
Abbreviations
AUC: area under the curve; BMI: body mass index; CEA: carcinoembryonic antigen; CI: confidence interval; CD: Clavien-Dindo; CRP: C-reactive protein; HR: hazard ratio; OS: overall survival; PNI: Prognostic nutritional index; pStage: pathological stage; ROC: Receiver operating characteristic; TNM: tumor, node, metastasis.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
References
1. Matsumoto S, Takayama T, Wakatsuki K, Tanaka T, Migita K, Ito M, Nakajima Y. Palliative Surgery for Gastric Cancer with Gastric Outlet Obstruction or Anemia due to Tumor Bleeding. Hepatogastroenterology. 2015; 62:1041–46. [PubMed].
2. Reyes López A, Gómez Camacho F, Gálvez Calderón C, Miño Fugarolas G. Iron-deficiency anemia due to chronic gastrointestinal bleeding. Rev Esp Enferm Dig. 1999; 91:345–58. [PubMed].
3. Hirahara N, Tajima Y, Fujii Y, Kaji S, Kawabata Y, Hyakudomi R, Yamamoto T. High Preoperative Prognostic Nutritional Index Is Associated with Less Postoperative Complication-Related Impairment of Long-Term Survival After Laparoscopic Gastrectomy for Gastric Cancer. J Gastrointest Surg. 2020; 24:2852–55. https://doi.org/10.1007/s11605-020-04737-w. [PubMed].
4. Han WH, Oh YJ, Eom BW, Yoon HM, Kim YW, Ryu KW. Prognostic impact of infectious complications after curative gastric cancer surgery. Eur J Surg Oncol. 2020; 46:1233–38. https://doi.org/10.1016/j.ejso.2020.04.032. [PubMed].
5. Yang Y, Gao P, Song Y, Sun J, Chen X, Zhao J, Ma B, Wang Z. The prognostic nutritional index is a predictive indicator of prognosis and postoperative complications in gastric cancer: A meta-analysis. Eur J Surg Oncol. 2016; 42:1176–82. https://doi.org/10.1016/j.ejso.2016.05.029. [PubMed].
6. Sasahara M, Kanda M, Ito S, Mochizuki Y, Teramoto H, Ishigure K, Murai T, Asada T, Ishiyama A, Matsushita H, Tanaka C, Kobayashi D, Fujiwara M, et al. The Preoperative Prognostic Nutritional Index Predicts Short-Term and Long-Term Outcomes of Patients with Stage II/III Gastric Cancer: Analysis of a Multi-Institution Dataset. Dig Surg. 2020; 37:135–44. https://doi.org/10.1159/000497454. [PubMed].
7. Kiuchi J, Komatsu S, Kosuga T, Kubota T, Okamoto K, Konishi H, Shiozaki A, Fujiwara H, Ichikawa D, Otsuji E. Long-term Postoperative Nutritional Status Affects Prognosis Even After Infectious Complications in Gastric Cancer. Anticancer Res. 2018; 38:3133–38. https://doi.org/10.21873/anticanres.12575. [PubMed].
8. Watanabe H, Hayashi T, Komori K, Hara K, Maezawa Y, Kano K, Shimoda Y, Fujikawa H, Aoyama T, Yamada T, Yamamoto N, Cho H, Ito H, et al. Impact of Postoperative Complications on Recurrence in Patients With Stage II/III Gastric Cancer Who Received Adjuvant Chemotherapy With S-1. Anticancer Res. 2020; 40:1683–90. https://doi.org/10.21873/anticanres.14120. [PubMed].
9. Onodera T, Goseki N, Kosaki G. [Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients]. Nihon Geka Gakkai Zasshi. 1984; 85:1001–05. [PubMed].
10. Murri AM, Hilmy M, Bell J, Wilson C, McNicol AM, Lannigan A, Doughty JC, McMillan DC. The relationship between the systemic inflammatory response, tumour proliferative activity, T-lymphocytic and macrophage infiltration, microvessel density and survival in patients with primary operable breast cancer. Br J Cancer. 2008; 99:1013–19. https://doi.org/10.1038/sj.bjc.6604667. [PubMed].
11. Englund A, Molin D, Enblad G, Karlén J, Glimelius I, Ljungman G, Amini RM. The role of tumour-infiltrating eosinophils, mast cells and macrophages in Classical and Nodular Lymphocyte Predominant Hodgkin Lymphoma in children. Eur J Haematol. 2016; 97:430–38. https://doi.org/10.1111/ejh.12747. [PubMed].
12. Tanaka A, Sakaguchi S. Regulatory T cells in cancer immunotherapy. Cell Res. 2017; 27:109–18. https://doi.org/10.1038/cr.2016.151. [PubMed].
13. Joshi NS, Akama-Garren EH, Lu Y, Lee DY, Chang GP, Li A, DuPage M, Tammela T, Kerper NR, Farago AF, Robbins R, Crowley DM, Bronson RT, Jacks T. Regulatory T Cells in Tumor-Associated Tertiary Lymphoid Structures Suppress Anti-tumor T Cell Responses. Immunity. 2015; 43:579–90. https://doi.org/10.1016/j.immuni.2015.08.006. [PubMed].
14. Mirili C, Yılmaz A, Demirkan S, Bilici M, Basol Tekin S. Clinical significance of prognostic nutritional index (PNI) in malignant melanoma. Int J Clin Oncol. 2019; 24:1301–10. https://doi.org/10.1007/s10147-019-01461-7. [PubMed].
15. Liao G, Zhao Z, Yang H, Chen M, Li X. Can Prognostic Nutritional Index be a Prediction Factor in Esophageal Cancer?: A Meta-Analysis. Nutr Cancer. 2020; 72:187–93. https://doi.org/10.1080/01635581.2019.1631859. [PubMed].
16. Li B, Lu Z, Wang S, Hou J, Xia G, Li H, Yin B, Lu W. Pretreatment elevated prognostic nutritional index predicts a favorable prognosis in patients with prostate cancer. BMC Cancer. 2020; 20:361. https://doi.org/10.1186/s12885-020-06879-1. [PubMed].
17. Hayashi T, Yoshikawa T, Aoyama T, Hasegawa S, Yamada T, Tsuchida K, Fujikawa H, Sato T, Ogata T, Cho H, Oshima T, Rino Y, Masuda M. Impact of infectious complications on gastric cancer recurrence. Gastric Cancer. 2015; 18:368–74. https://doi.org/10.1007/s10120-014-0361-3. [PubMed].
18. Wang S, Xu L, Wang Q, Li J, Bai B, Li Z, Wu X, Yu P, Li X, Yin J. Postoperative complications and prognosis after radical gastrectomy for gastric cancer: a systematic review and meta-analysis of observational studies. World J Surg Oncol. 2019; 17:52. https://doi.org/10.1186/s12957-019-1593-9. [PubMed].
19. Li QG, Li P, Tang D, Chen J, Wang DR. Impact of postoperative complications on long-term survival after radical resection for gastric cancer. World J Gastroenterol. 2013; 19:4060–65. https://doi.org/10.3748/wjg.v19.i25.4060. [PubMed].
20. Zhao B, Zhang J, Zhang J, Zou S, Luo R, Xu H, Huang B. The Impact of Preoperative Underweight Status on Postoperative Complication and Survival Outcome of Gastric Cancer Patients: A Systematic Review and Meta-analysis. Nutr Cancer. 2018; 70:1254–63. [PubMed].
21. Bottomley MJ, Harden PN. Update on the long-term complications of renal transplantation. Br Med Bull. 2013; 106:117–34. https://doi.org/10.1093/bmb/ldt012. [PubMed].
22. Basu P, Goldenberg A, Cowan N, Eilers R, Hau J, Jiang SIB. A 4-year retrospective assessment of postoperative complications in immunosuppressed patients following Mohs micrographic surgery. J Am Acad Dermatol. 2019; 80:1594–601. https://doi.org/10.1016/j.jaad.2018.11.032. [PubMed].
23. Ikuta S, Miki C, Tanaka K, Konishi N, Mohri Y, Tonouchi H, Kusunoki M. Serum immunosuppressive acidic protein as an interleukin-6 related index of deteriorating condition in gastric cancer patients. Dig Surg. 2003; 20:532–38. https://doi.org/10.1159/000073700. [PubMed].
24. Quan L, Gong Z, Yao S, Bandera EV, Zirpoli G, Hwang H, Roberts M, Ciupak G, Davis W, Sucheston L, Pawlish K, Bovbjerg DH, Jandorf L, et al. Cytokine and cytokine receptor genes of the adaptive immune response are differentially associated with breast cancer risk in American women of African and European ancestry. Int J Cancer. 2014; 134:1408–21. https://doi.org/10.1002/ijc.28458. [PubMed].
25. Felekis D, Eleftheriadou A, Papadakos G, Bosinakou I, Ferekidou E, Kandiloros D, Katsaragakis S, Charalabopoulos K, Manolopoulos L. Effect of perioperative immuno-enhanced enteral nutrition on inflammatory response, nutritional status, and outcomes in head and neck cancer patients undergoing major surgery. Nutr Cancer. 2010; 62:1105–12. https://doi.org/10.1080/01635581.2010.494336. [PubMed].
26. Zhao H, Zhao H, Wang Y, Jing H, Ding Q, Xue J. Randomized clinical trial of arginine-supplemented enteral nutrition versus standard enteral nutrition in patients undergoing gastric cancer surgery. J Cancer Res Clin Oncol. 2013; 139:1465–70. https://doi.org/10.1007/s00432-013-1466-5. [PubMed]. Retraction in: J Cancer Res Clin Oncol. 2015; 141:573. https://doi.org/10.1007/s00432-015-1913-6. [PubMed].
27. Margonis GA, Sasaki K, Andreatos N, Nishioka Y, Sugawara T, Amini N, Buettner S, Hashimoto M, Shindoh J, Pawlik TM. Prognostic impact of complications after resection of early stage hepatocellular carcinoma. J Surg Oncol. 2017; 115:791–804. https://doi.org/10.1002/jso.24576. [PubMed].
28. Tu RH, Lin JX, Li P, Xie JW, Wang JB, Lu J, Chen QY, Cao LL, Lin M, Zheng CH, Huang CM. Prognostic significance of postoperative pneumonia after curative resection for patients with gastric cancer. Cancer Med. 2017; 6:2757–65. https://doi.org/10.1002/cam4.1163. [PubMed].
29. Hirahara N, Matsubara T, Fujii Y, Kaji S, Hyakudomi R, Yamamoto T, Uchida Y, Miyazaki Y, Ishitobi K, Kawabata Y, Tajima Y. Geriatric nutritional risk index as a prognostic marker of pTNM-stage I and II esophageal squamous cell carcinoma after curative resection. Oncotarget. 2020; 11:2834–46. https://doi.org/10.18632/oncotarget.27670. [PubMed].
30. Pan QX, Su ZJ, Zhang JH, Wang CR, Ke SY. A comparison of the prognostic value of preoperative inflammation-based scores and TNM stage in patients with gastric cancer. Onco Targets Ther. 2015; 8:1375–85. https://doi.org/10.2147/OTT.S82437. [PubMed].
31. Maeda K, Shibutani M, Otani H, Nagahara H, Ikeya T, Iseki Y, Tanaka H, Muguruma K, Hirakawa K. Inflammation-based factors and prognosis in patients with colorectal cancer. World J Gastrointest Oncol. 2015; 7:111–17. https://doi.org/10.4251/wjgo.v7.i8.111. [PubMed].
32. Park SH, Lee S, Song JH, Choi S, Cho M, Kwon IG, Son T, Kim HI, Cheong JH, Hyung WJ, Choi SH, Noh SH, Choi YY. Prognostic significance of body mass index and prognostic nutritional index in stage II/III gastric cancer. Eur J Surg Oncol. 2020; 46:620–25. https://doi.org/10.1016/j.ejso.2019.10.024. [PubMed].
33. Gao ZM, Wang RY, Deng P, Ding P, Zheng C, Hou B, Li K. TNM-PNI: a novel prognostic scoring system for patients with gastric cancer and curative D2 resection. Cancer Manag Res. 2018; 10:2925–33. https://doi.org/10.2147/CMAR.S169206. [PubMed].
34. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer. 2017; 20:1–19. https://doi.org/10.1007/s10120-016-0622-4. [PubMed].
35. Sobin L, Gospodarowicz M, Wittekind C, editors. International Union Against Cancer (UICC). TNM classification of malignant tumors, 7th ed. New York: Wiley-Blackwell; 2010.
36. Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, de Santibañes E, Pekolj J, Slankamenac K, Bassi C, Graf R, Vonlanthen R, Padbury R, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009; 250:187–96. https://doi.org/10.1097/SLA.0b013e3181b13ca2. [PubMed].