
INTRODUCTION
Ostesarcoma is a rare, aggressive sarcoma. Whereas there is an agreement that surgery, with adjuvant chemotherapy, is paramount for the primary therapy of the cancer, about 30% of patients without evident metastases at presentation will die of disease [1]. The prognosis is even poorer (10% survival at 5-years) in patients with synchronous metastases [1]. Therefore there is an urgent need to identify new targets, different risk groups and predictive factors for tailored treatment for each individual.
Various mechanisms have been proposed for the resistance of human solid tumors to immune recognition and obliteration, including the recruitment of regulatory T cells (T-reg), myeloid derived suppressor cells (MDSC) [2] and up-regulation of immune inhibitory ligands, such as the ligand of programmed cell death protein 1 (PD-L1) [3].
T-lymphocyte and antigen-presenting cells (APCs) interaction is in fact bi-directional and mediated by PD-L1 and programmed cell death protein 1 (PD1) on APCs and on lymphocytes. PD-L1 is expressed also by several tumors [3].
PD1/PD-L1 pathway inhibitors such as pembrolizumab, nivolumab, atezolizumab have been approved from several solid tumors (melanoma, kidney, lung cancer, head and neck, Merkel cell tumors, Hodgkin’s lymphoma), and PD-L1 expression on tumoral cells (TC) or in immune-infiltrate (IC) has been associated with response to checkpoint inhibitors, in some cases [4], but PD-L1 expression predictive value remain controversial [5, 6]. Recently, anecdotal responses with pembrolizumab, nivolumab and also with nivolumab/pazopanib combination were reported in osteosarcoma patients [7–9]. These compounds interrupt PD-1/PD-L1 axis, impeding the PD-L1 mediated ‘tumor shield’ effect (Figure 1).
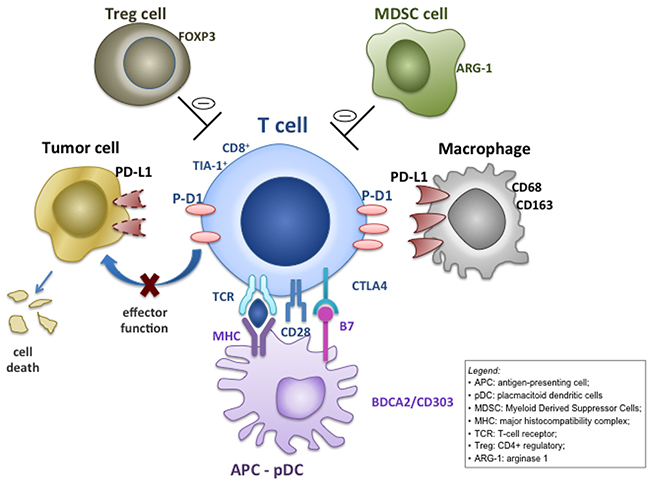
Figure 1: Mechanisms for intratumoral programmed cell death ligand-1 (PD-L1) expression. Adaptive focal expression of PD-L1 by macrophages (CD68+/CD163+) occurs at the interface of tumor cell nests with immune infiltrates secreting pro-inflammatory factors such as interferon-γ. The ligation of PD-L1 on macrophage and, in some histotypes, on tumor cells, with programmed cell death protein 1 (PD-1) molecules will down-modulate T cell function, essentially creating a negative feedback loop that reduces antitumor immunity (the so called ‘tumor shield’ effect), eventually reducing CD8 tumoricidal function.
Few data on osteosarcoma microenvironment composition and the PD-1/PD-L1 expression are available, and most of the studies refer to small series with incomplete clinical information, inhomogeneous for stage (metastatic and localized patients), treatments and timing of biopsies [10].
The present study aim is to characterize the immune-infiltrates and PD-L1/PD-1 pathway in sample of chemo-naïve patients with localized osteosarcoma, treated according to the same protocol, in order to assess its prognostic implications and its potential role in cancer immune-evasion.
RESULTS
Tumoral microenvironment components prior chemotherapy (bioptic samples)
Eighty-six out of 129 cases analysed were evaluable for at least 7 markers and were included in the present study.
Most of the cases presented TILs (CD3+ 77/86, 90%; CD8+ 74/86, 86%, CD20+ 25/86, 29%), while FOXP3+ (Treg) were detected in 28/86 (33%) of the patients (Table 1; Figure 2). Tia-1 was detected in 57/78 (73%) of the samples. TAMs (CD163 positive) were observed in the microenvironment in 47/70 (67%) of the patients, while 31/74 (37%) patients presented also high levels of CD68 positivity (Table 1; Figure 2). Only 3/78 (4%) and 16/78 (21%) cases presented CD303+ and Arginase-1+ cells. PD-L1 expression was found in 12/86 (14%) patients in IC and 0/86 (0%) in TC; 19/86 (22%) showed PD-1 expression in IC (Table 1; Figure 2).
Table 1: Immunological characterization of tumor microenvironment in 86 patients with localized osteosarcoma
|
CD3 |
CD8 |
CD20 |
FOXP3 |
Tia1 |
CD68* |
CD163 |
CD303 |
Arg-1 |
PD-L1 |
PD-1 |
PD-L1 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
Pos |
77 (90) |
74 (86) |
25 (29) |
28 (33) |
57 (73) |
31 (37) |
47 (67) |
3 (4) |
16 (21) |
0 (0) |
19 (22) |
12 (14) |
Neg |
9 (10) |
12 (14) |
61 (71) |
58 (67) |
21 (27) |
53 (63) |
23 (33) |
75 (96) |
62 (79) |
86 (100) |
67 (78) |
74 (86) |
Arg-1: Arginase-1; TC: tumor cells; IC: immune cells; * CD-68: Pos: high level expression; neg: low level expression.
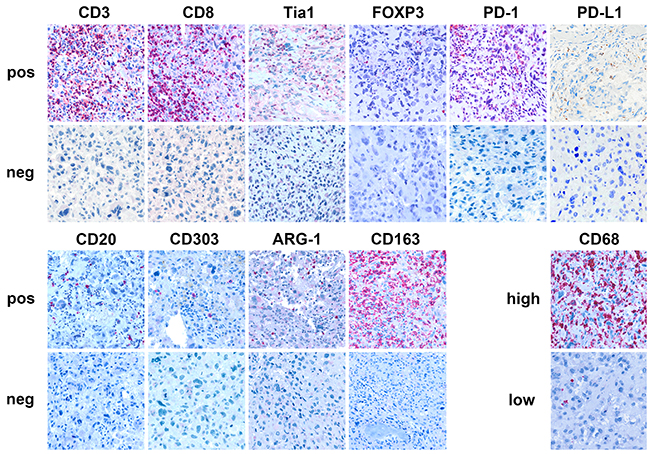
Figure 2: Tumor microenvironment in localized osteosarcoma. Immunohistochemical expression of CD3, CD8, CD20 (T tumor infiltrating lymphocytes: TILs), Tia-1 (cytotoxic T cell), FOXP3 (T regulatory lymphocytes: T-regs), PD-1, PD-L1, CD68 (tumor associated macrophages: TAM), BDCA-2/CD303 (plasmacytoid dendritic cells: pDC), Arginase-1 (myeloid derived suppressor cells: MDSC) proteins.
Survival analysis
With a median follow-up of 8 years (range 1-13), the 5-year OS was 74% (95% CI 64-85). Univariate analysis showed better 5-year OS for good responders (good 89% vs poor 57%, p = 0.0001), for cases with CD8/Tia1 tumoral infiltrates (CD8+/Tia1+ 81% vs CD8+/Tia1- 60% vs CD8-/Tia1- 45%, p = 0.002) and patients with normal AP at baseline (AP normal 85% vs AP high 44%, p = 0.04) (Table 2, Figure 3). No statistically significant difference was observed in 5-year OS according to PD-1, FOXP3, CD68, CD20, Arginase-1, CD303, CD163 expression in microenvironment, and age, gender or LDH, while PD-L1 (IC) positive cases had a non-significant inferior 5-year OS (PD-L1+ 58% vs PD-L1- 77%, p = 0.14) (Table 2).
Table 2: Univariate Analysis for Overall Survival (OS) in patients with localized osteosarcoma
Pts N. |
% 5-year OS |
95% CI |
P-value |
|
|---|---|---|---|---|
Overall |
86 |
74.5 |
65-84 |
|
Age |
0.9 |
|||
≥ 18 years |
27 |
74 |
57-90 |
|
< 18 years |
59 |
75 |
63-86 |
|
Sex |
0.8 |
|||
Female |
33 |
76 |
61-90 |
|
Male |
53 |
74 |
61-89 |
|
Histologic Response° |
0.0001 |
|||
Good |
45 |
89 |
80-98 |
|
Poor |
40 |
57 |
42-73 |
|
CD8 |
0.003 |
|||
Positive |
74 |
78 |
69-88 |
|
Negative |
12 |
50 |
22-78 |
|
TIA-1 °° |
0.008 |
|||
Moderate |
14 |
86 |
67-100 |
|
Focal |
43 |
79 |
67-91 |
|
None |
21 |
52 |
31-74 |
|
CD8/ Tia1 °° |
0.002 |
|||
Positive / Positive |
57 |
81 |
70-91 |
|
Positive / Negative |
10 |
60 |
30-90 |
|
Negative / Negative |
11 |
45 |
16-75 |
|
CD3 |
0.07 |
|||
Positive |
77 |
78 |
69-87 |
|
Negative |
9 |
44 |
12-77 |
|
FOXP3 * |
0.13 |
|||
Positive |
28 |
75 |
54-93 |
|
Negative |
56 |
73 |
64-85 |
|
PD-1 (IC) |
0.6 |
|||
Positive |
19 |
74 |
54-93 |
|
Negative |
67 |
74 |
64-85 |
|
PD-L1 (IC) |
0.14 |
|||
Positive |
12 |
58 |
30-86 |
|
Negative |
74 |
77 |
67-87 |
|
LDH °° |
0.15 |
|||
Normal |
60 |
78 |
68-89 |
|
High |
18 |
61 |
39-84 |
|
sAP |
0.04 |
|||
Normal |
48 |
85 |
75-95 |
|
High |
38 |
64 |
48-80 |
|
Arginase-1 ** |
0.3 |
|||
Positive |
16 |
81 |
62-100 |
|
Negative |
61 |
70 |
59-82 |
|
CD303 °° |
0.9 |
|||
Positive |
3 |
67 |
13-100 |
|
Negative |
75 |
73 |
63-83 |
|
CD68 * |
0.1 |
|||
High |
31 |
84 |
71-99 |
|
Low |
53 |
67 |
54-80 |
|
CD163 *** |
0.17 |
|||
Positive |
47 |
81 |
70-92 |
|
Negative |
23 |
56 |
36-77 |
° Not available in 1 patient; °° non available in 8 patients; * not available in 2 patients; ** not available in 7 patients; *** not available in 16 patients
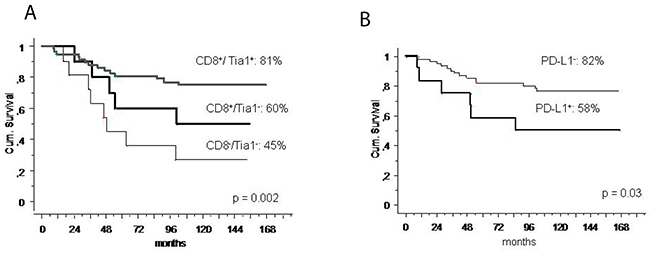
Figure 3: Survival and immune-infiltrate. (A) 5-year overall survival according to CD8/Tia1 expression in localized osteosarcoma; (B) 5-year overall survival according to PD-L1 expression in patients with CD8+ localized osteosarcoma.
Table 3: Multivariate Analysis for Overall Survival (OS) in patients with localized osteosarcoma
Variable |
RR |
95% CI |
P |
|---|---|---|---|
CD8/Tia1 |
|||
Positive/Positive |
1 |
0.05 |
|
Positive/Negative |
1.8 |
0.7-5.2 |
0.2 |
Negative/Negative |
3.1 |
1.2-7.8 |
0.01 |
Histologic Response |
|||
Poor |
1 |
0.007 |
|
Good |
0.27 |
0.1-0.7 |
|
sPA |
|||
Normal |
1 |
0.2 |
|
High |
1.75 |
0.8-3.9 |
After multivariate analysis, good histologic response (p = 0.007) and a CD8+/Tia1+ lymphocytic infiltrate (0.05) were independently associated with better survival (Table 3).
Since PD-L1(IC) is a marker of cytotoxic function exhaustion, we investigated if PD-L1 expression could influence survival in the subgroup of patient with CD8+ lymphocytes: at univariate analysis the 5-year OS was 82% (95%CI 73%-92%) in case of PD-L1 negative and 58% (95% CI 34%-78%) in positive PD-L1 (p = 0.03) (Figure 3). At the multivariate analysis in this subgroup, lack of PD-L1 was and independent prognostic factor for longer survival (p = 0.04) (Table 4).
Table 4: Multivariate Analysis for Overall Survival in patients with CD8+ localized osteosarcoma
Variable |
RR |
95% CI |
P |
|---|---|---|---|
PD-L1 |
|||
Negative |
1 |
0.04 |
|
Positive |
2.8 |
1-7.4 |
|
Histologic Response |
|||
Poor |
1 |
0.02 |
|
Good |
0.3 |
0.1-0.9 |
|
sPA |
|||
Normal |
1 |
0.5 |
|
High |
1.4 |
0.5-3.8 |
Tumoral microenvironment components post-induction chemotherapy (surgical samples)
Based on multivariate analysis results on pre-treatment samples, a post-hoc analysis on CD8 and Tia1 was performed.
Due to post-treatment changes 33/86 patients were assessable after treatment (excluding 53 patients with massive necrosis and no tumor).
Chemotherapy-induced changes of CD8+ TILs were as follow: all patients with score 0 (5 cases) were unchanged, the proportion of patients with score 1 decreased: 19/33 (58%) pre-chemotherapy, 14/33 (42%) post-treatment; and the proportion of patients with a score 2/3 increased: 9/33 (27%) to 12/33 (36%) (p 0.5).
A survival analysis according to presence of CD8+ /Tia1+ infiltrates presence in the surgical samples after induction-chemotherapy, confirmed their prognostic role: 5- year OS was 78% (CI% 51-100) for CD8+/Tia1+ (22 patients), 64% (CI%43-84) for CD8+/Tia1- (9 patients) and none was alive with CD8-/Tia1- (2 patients) (p 0.05) (Supplementary Figure 1).
DISCUSSION
The role of microenvironment in tumor immune escape is well recognized. Several studies addressed the role of tumor microenvironment in pathobiology and its impact on survival of osteosarcoma [11–15], however none is specific for osteosarcoma in the localized stage, nor compared the prognostic power of immune-infiltrate with the other validate prognostic factor routinely used in clinical practice [16, 17],
The present study, including patients with osteosarcoma in a localized stage, and treated within the same protocol [16], demonstrated an independent prognostic role of CD8+ and Tia1 lymphocytes.
The first study demonstrating the association between CD8 infiltrate and cancer specific survival was published in 2001 [18], and similar findings were subsequently confirmed among many histotypes [19, 20].
In the sarcoma field both a series of 33 ostesarcoma, including metastastic and localised patients [11], and a large soft tissue sarcoma French study, including several histotypes and also low grades lesions, failed to demonstrate a prognostic role for CD8+ lymphocytes [21].
The results of our study are in contrast with those data [11, 21], in fact a strong advantage in terms of survival has been observed in patients with CD8+ infiltrate.
To investigate the differentiation state of tumor-infiltrating T cells, tissues were analyzed for Tia1 expression, which is a marker of cytotoxic function: the prognostic significance of CD8+ cells was even more relevant when the tumor infiltrate was characterized by the concomitant presence of Tia1+ lymphocytes. Tia1+ lymphocytes might represent a more efficient subset of CD8+ effector cells, playing an important role in immune-surveillance of osteosarcoma [22].
The prognostic role of cytotoxic TILs CD8/Tia1 was also confirmed after induction chemotherapy, while chemotherapy does not seem to induce significant changes in CD8+ TILs: all cases with no CD8+ TILs prior chemotherapy, were confirmed negative after chemotherapy, while a slight increase on score severity (1 to 2/3) was observed.
In our study, the rate of PD-L1 expression in IC was 14%. Previous studies on osteosarcoma samples reported a higher rate of positive expression of PD-L1(IC) ranging from 25% [11] to 74% [10]. This difference might be related to the heterogeneity of the cases examined, being many of them metastatic, while our patients all had localized disease. In fact, it is well known that PD-L1 expression increases in advanced stages of the diseases as reported by Sundara Y et al: 13% in primary tumours, 25% in local relapses tissue and 48% in metastatic (p = 0.002) [12].
In our study a trend towards an inferior survival for positive PD-L1(IC) patients was observed. Other reports were able to demonstrate a significantly inferior event-free-survival (EFS) for osteosarcoma patients with positive PD-L1(IC) [11]. A prognostic role for PD-L1 was also confirmed by Kim et al, at RNA level [10]. Interestingly, in our series, the PD-L1(IC) expression has a prognostic significance at multivariate analysis in the subgroup of patients with CD8+ immune-infiltrate. It might be hypothesised that “PD-L1”-mediated immune-suppression negatively influences CD8+ lymphocytes function (Figure 1). In addition, it was shown that tumor response to PD-L1 or PD-1 inhibition is directly related to both the level of PD-L1 expression and lymphocytic infiltration of the tumor [23–25].
None of the patients had PD-L1 on tumor cells, as shown for other histotypes, such as colon rectal and gastric carcinoma [26, 27]. About 7% of osteosarcoma presented PD-L1 in the neoplastic clone in the study by Koirala et al [11], while head and neck squamous cell carcinoma, melanoma, breast and kidney cancer frequently express PD-L1 on the surface of tumour [4, 28]. Such variable expression among different studies may reflect the variable susceptibility of tumour cells and infiltrating immune cells to cytokines and other stromal factors in the tumour milieu [5]. In fact there are two distinct type of PD-L1 expression: the first is a constitutive (innate) expression on tumoral cells membranes, with an homogenous patter; the second is adaptative, and can be found both on tumoral cells or in macrophage [5].
In 67% of the cases we found CD163+ macrophages in microenvironment. CD163 was shown to be a useful marker for M2-like macrophages, which have a “pro-tumoral” activity, in contrast with M1-like macrophages characterized by a “tumoricidal” activity [29].
In our series no difference in survival according with presence of TAMs, characterized by both CD163 and CD68 expression, was observed (CD163+ 81% vs CD163- 56%, p = 0.17), while in other osteosarcoma series a prognostic role of TAMs was suggested [13, 14]. This might be explained by different statistical analysis design and different stages of patients included [13, 14].
Our data suggest a role of immune-infiltrate in progression of localized osteosarcoma, and might support the use of immune-modulating agents in the treatment of this tumor. Of interest, mifamurtide, a modulator of innate immunity, which increases a wide variety of immunomodulatory molecules [15] and favours CD8 and NK cell activation [30], has been approved by EMA for the treatment of patients with localized high-grade osteosarcoma based on the results of a randomized trial [31].
In conclusion, CD8/Tia1 citotoxic T-lymphocytes emerge as an important player in anti-tumor immune response. Also, this study highlights the prognostic role of tumor microenvironment in the setting of localized osteosarcoma. The data are interesting and intriguing, but a clinical application requires confirmations in other series (Figure 4).
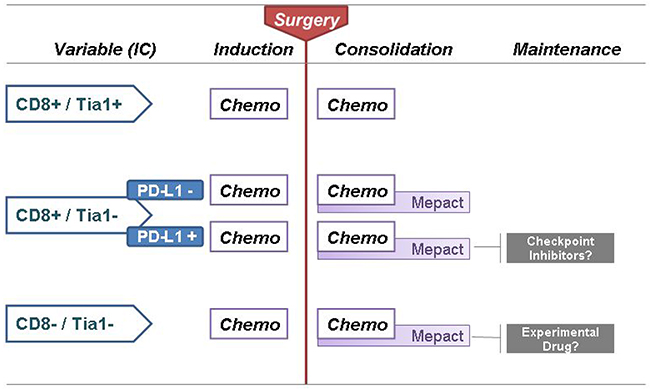
Figure 4: Proposal for ‘Immune-infiltrate based treatment algorithm’ for localized osteosarcoma.
MATERIALS AND METHODS
Pre-treatment (bioptic samples)
After EC approval, tissue samples obtained from biopsies performed prior chemotherapy in 129 patients were collected. Patients were prospectively treated at Istituto Ortopedico Rizzoli from 04/2001 to 11/2006 within protocol ISG-OS1, with surgery and a chemotherapy based on methotrexate, cispaltin, adriamicyn and ifosfamide as described [16].
The clinical characteristics of the patients were the following: the median age was 16 years (range 4-39 years), with paediatric patients (59/86, 67%) and male gender (53/86, 62%) being most represented. High LDH levels and high AP at baseline were detected in 36/86 (42%) and 18/86 (21%) of patients respectively. All patients underwent neo-adjuvant chemotherapy and surgery as per protocol. A good pathologic response (≥90% necrosis) was achieved by 45/86 (52%) of the patients.
All samples underwent decalcification as previously described [17].
For tissue microarray (TMA) construction, a slide stained with hematoxylin and eosin was prepared from each formalin-fixed, paraffin-embedded (FFPE), and representative tumor regions were morphologically identified and marked on each slide. Tissue cylinders with a diameter of 1.0 mm were punched from the marked areas of each block and brought into a recipient paraffin block. Five TMAs were constructed. Each tumor sample was represented by a minimum of 1 core to a maximum of 5 cores.
From TMA blocks, 4 micron-sections were cut. This histological sections were coloured with haematoxylin eosin and the tumor microenvironment was characterized by applying antibodies directed against fixation resistant epitopes of CD68 (tumor associated macrophages: TAM), CD3, CD8, CD20 (T tumor infiltrating lymphocytes: TILs), FOXP3 (T regulatory lymphocytes: T-regs), Tia-1 (cytotoxic T cell), BDCA-2/CD303 (plasmacytoid dendritic cells: pDC), Arginase-1 (myeloid derived suppressor cells: MDSC) proteins. PD-1 expression on immune-cells (IC), and PD-L1 on both tumour cells (TC) and IC was also investigated. The antibody reactivity, source as well as the antigen retrieval protocols were reported in Supplementary Table 1.
A semi-quantitative score from 0 to 3 was assigned to immune infiltrates: 0 = “none”: no immune infiltrates; 1 = “focal”: mostly perivascular in tumor with some intra-tumoral extension; 2 = “moderate”: prominent extension of immune infiltrates away from perivascular areas and amongst tumor cells); 3 = “severe” (immune infiltrates obscuring tumor) [4]. Pathologists were blinded to clinical information.
Only cores with tumoral component were included in the analysis. The immunehistochemical scores were generally concordant among cores of the same patient, in case of heterogeneity the highest score was considered for the analysis.
For survival analysis samples were classified as negative (immunostaining = 0) or positive (immunostaining = 1 to 3) for all markers except: CD68+ cases that were classified in high expressing (severe and moderate expression) and low expressing (focal expression). Score for PD-L1 expression in TC: specimens with >5% membranous expression were considered positive.
The following factors were correlated with overall survival (OS): age (pediatric < 18 years vs adult ≥ 18 years), gender, LDH and phosphatase alkaline (PA) levels at baseline (normal vs high), pathologic response (good: chemotherapy-induced tumor necrosis ≥ 90%; poor: chemotherapy-induced tumor necrosis < 90%) [17], tumoral microenvironment components, PD-1 expression on IC, and PD-L1 both on TC and IC.
OS was estimated according to the Kaplan and Meier method with their respective 95% confidence intervals (CI) and calculated from the first day of chemotherapy administration to death or last follow-up visit.
Post-induction chemotherapy (surgical samples)
In 86/129 patients, FFPE from tumoral masses surgically resected, after neoadjuvant chemotherapy, were collected. The full slides sections from FFPA were investigate by immunohistochemistry for CD8+ and Tia1 expression.
The following factors were correlated with overall survival: tumoral microenvironment components (CD8 and Tia1).
Abbreviations
TMAs: tissue microarrays; Pts: patients; TAM: tumor associated macrophage; pDC: plasmacytoid dendritic cells; MDSC: myeloid derived suppressor cells; IC: immune-cells; AP: alkaline phosphatase; 5-year OS: 5-year overall survival; PD-1: programmed cell death 1; PD-L1: programmed cell death-ligand 1; APCs: antigen-presenting cells
Author contributions
EP, CA substantive intellectual contribution to conception and design of study, drafting and revision of manuscript, statistical analyses and interpretation of data
SF: patients selection / inclusion; statistical analyses and interpretation of data
SP, PL, PP: substantive intellectual contribution to conception and design of study, final approval of the version to be published
MT, KS, ALMSB: drafting and revision of manuscript
ACKNOWLEDGMENTS
The authors thank Alba Balladelli and Cristina Ghinelli for editing support, and Ayse U. Akarca for PD-L1 staining.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
FUNDING
European Project EuroSarc FP7 and Matteo Amitrano Association
REFERENCES
1. Mirabello L, Troisi RJ, Savage SA. Osteosarcoma incidence and survival rates from 1973 to 2004: data from the surveillance, epidemiology, and end results program. Cancer. 2009; 115:1531–1543.
2. Gabrilovich DI, Nagaraj S. Myeloid-derived suppressor cells as regulators of the immune system. Nat Rev Immunol. 2009; 9:162–174.
3. Topalian SL, Taube JM, Anders RA, Pardoll DM. Mechanism-driven biomarkers to guide immune checkpoint blockade in cancer therapy. Nat Rev Cancer. 2016; 16:275–287.
4. Taube JM, Klein A, Brahmer JR, Xu H, Pan X, Kim JH, Chen L, Pardoll DM, Topalian SL, Anders RA. Association of PD-1, PD-1 ligands, and other features of the tumor immune microenvironment with response to anti–PD-1 therapy. Clin Cancer Res. 2014; 20:5064–5074.
5. Topalian SL, Hodi FS, Brahmer JR, Gettinger SN, Smith DC, McDermott DF, Powderly JD, Carvajal RD, Sosman JA, Atkins MB, Leming PD, Spigel DR, Antonia SJ, et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med. 2012; 366:2443–2454.
6. McDermott DF, Sosman JA, Sznol M, Massard C, Gordon MS, Hamid O, Powderly JD, Infante JR, Fassò M, Wang YV, Zou W, Hegde PS, Fine GD, et al. Atezolizumab, an anti-programmed death-ligand 1 antibody, in metastatic renal cell carcinoma: long-term safety, clinical activity, and immune correlates from a phase ia study. J Clin Oncol. 2016; 34:833–842.
7. Paoluzzi L, Cacavio A, Ghesani M, Karambelkar A, Rapkiewicz A, Weber J, Rosen G. Response to anti-PD1 therapy with nivolumab in metastatic sarcomas. Clin Sarcoma Res. 2016; 6:24.
8. Tawbi H, Burgess MA, Crowley J, Van Tine BA, Hu J, Schuetze S. Safety and efficacy of PD-1 blockade using pembrolizumab in patients with advanced soft tissue (STS) and bone sarcomas (BS): results of SARC028 - A multicenter phase II study. J Clin Oncol. 2016.
9. McCaughan GJ, Fulham MJ, Mahar A, Soper J, Hong AM, Stalley PD, Tattersall MH, Bhadri VA. Programmed cell death-1 blockade in recurrent disseminated Ewing sarcoma. J Hematol Oncol. 2016; 9:48.
10. Shen JK, Cote GM, Choy E, Yang P, Harmon D, Schwab J, Nielsen GP, Chebib I, Ferrone S, Wang X, Wang Y, Mankin H, Hornicek FJ, et al. Programmed cell death ligand 1 expression in osteosarcoma. Cancer Immunol Res. 2014; 2:690–698.
11. Koirala P, Roth ME, Gill J, Piperdi S, Chinai JM, Geller DS, Hoang BH, Park A, Fremed MA, Zang X, Gorlick R. Immune infiltration and PD-L1 expression in the tumor microenvironment are prognostic in osteosarcoma. Sci Rep. 2016; 6:30093.
12. Sundara YT, Kostine M, Cleven AH, Bovée JV, Schilham MW, Cleton-Jansen AM. Increased PD-L1 and T-cell infiltration in the presence of HLA class I expression in metastatic high-grade osteosarcoma: a rationale for T-cell-based immunotherapy. Cancer Immunol Immunother. 2017; 66:119–128.
13. Dumars C, Ngyuen JM, Gaultier A, Lanel R, Corradini N, Gouin F, Heymann D, Heymann MF. Dysregulation of macrophage polarization is associated with the metastatic process in osteosarcoma. Oncotarget 2016; 7:78343–78354. https://doi.org/10.18632/oncotarget.13055.
14. Buddingh EP, Kuijjer ML, Duim RA, Bürger H, Agelopoulos K, Myklebost O, Serra M, Mertens F, Hogendoorn PC, Lankester AC, Cleton-Jansen AM. Tumor-infiltrating macrophages are associated with metastasis suppression in high-grade osteosarcoma: a rationale for treatment with macrophage activating agents. Clin Cancer Res. 2011; 17:2110–2119.
15. Kleinerman ES, Jia SF, Griffin J, Seibel NL, Benjamin RS, Jaffe N. Phase II study of liposomal muramyl tripeptide in osteosarcoma: the cytokine cascade and monocyte activation following administration. J Clin Oncol. 1992; 10:1310–1316.
16. Ferrari S, Ruggieri P, Cefalo G, Tamburini A, Capanna R, Fagioli F, Comandone A, Bertulli R, Bisogno G, Palmerini E, Alberghini M, Parafioriti A, Linari A, et al. Neoadjuvant chemotherapy with methotrexate, cisplatin, and doxorubicin with or without ifosfamide in nonmetastatic osteosarcoma of the extremity: an Italian sarcoma group trial ISG/OS-1. J Clin Oncol. 2012; 30:2112–2118.
17. Picci P, Bacci G, Campanacci M, Gasparini M, Pilotti S, Cerasoli S, Bertoni F, Guerra A, Capanna R, Albisinni U, Galletti S, Gherlinzoni F, Calderoni P, et al. Histologic evaluation of necrosis in osteosarcoma induced by chemotherapy. Cancer. 1985; 56:1515–1521
18. Zhang L, Conejo-Garcia JR, Katsaros D, Gimotty PA, Massobrio M, Regnani G, Makrigiannakis A, Gray H, Schlienger K, Liebman MN, Rubin SC, Coukos G. Intratumoral T cells, recurrence, and survival in epithelial ovarian cancer. N Engl J Med. 2003; 348:203–213
19. Galon J, Costes A, Sanchez-Cabo F, Kirilovsky A, Mlecnik B, Lagorce-Pagès C, Tosolini M, Camus M, Berger A, Wind P, Zinzindohoué F, Bruneval P, Cugnenc PH, et al. Type, density, and location of immune cells within human colorectal tumors predict clinical outcome. Science. 2006; 313:1960–1964.
20. Salgado R, Denkert C, Demaria S, Sirtaine N, Klauschen F, Pruneri G, Wienert S, Van den Eynden G, Baehner FL, Penault-Llorca F, Perez EA, Thompson EA, Symmans WF, et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: recommendations by an International TILs Working Group 2014. Ann Oncol. 2015; 26:259–271.
21. Toulmonde M, Adam J, Bessede A, Velasco V, Brouste V. Integrative assessment of expression and prognostic value of PDL1, IDO, and kynurenine in 371 primary soft tissue sarcomas with genomic complexity. J Clin Oncol. 2016.
22. Kim JR, Moon YJ, Kwon KS, Bae JS, Wagle S, Kim KM, Park HS, Lee H, Moon WS, Chung MJ, Kang MJ, Jang KY. Tumor infiltrating PD1-positive lymphocytes and the expression of PD-L1 predict poor prognosis of soft tissue sarcomas. PLoS One. 2013; 8:e82870.
23. Afanasiev OK, Yelistratova L, Miller N, Nagase K, Paulson K, Iyer JG, Ibrani D, Koelle DM, Nghiem P. Merkel polyomavirus-specific T cells fluctuate with merkel cell carcinoma burden and express therapeutically targetable PD-1 and Tim-3 exhaustion markers. Clin Cancer Res. 2013; 9:5351–5360.
24. Herbst RS, Soria JC, Kowanetz M, Fine GD, Hamid O, Gordon MS, Sosman JA, McDermott DF, Powderly JD, Gettinger SN, Kohrt HE, Horn L, Lawrence DP, et al. Predictive correlates of response to the anti-PD-L1 antibody MPDL3280A in cancer patients. Nature. 2014; 515:563–567.
25. Tumeh PC, Harview CL, Yearley JH, Shintaku IP, Taylor EJ, Robert L, Chmielowski B, Spasic M, Henry G, Ciobanu V, West AN, Carmona M, Kivork C, et al. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature. 2014; 515:568−571.
26. Llosa NJ, Cruise M, Tam A, Wicks EC, Hechenbleikner EM, Taube JM, Blosser RL, Fan H, Wang H, Luber BS, Zhang M, Papadopoulos N, Kinzler KW, et al. The vigorous immune microenvironment of microsatellite instable colon cancer is balanced by multiple counter-inhibitory checkpoints. Cancer Discov. 2015; 5:43–51.
27. Lipson EJ, Sharfman WH, Drake CG, Wollner I, Taube JM, Anders RA, Xu H, Yao S, Pons A, Chen L, Pardoll DM, Brahmer JR, Topalian SL. Durable cancer regression off- treatment and effective reinduction therapy with an anti-PD-1 antibody. Clin. Cancer Res. 2013; 19:462–468.
28. Lyford-Pike S, Peng S, Young GD, Taube JM, Westra WH, Akpeng B, Bruno TC, Richmon JD, Wang H, Bishop JA, Chen L, Drake CG, Topalian SL, et al. Evidence for a role of the PD-1:PD-L1 pathway in immune resistance of HPV- associated head and neck squamous cell carcinoma. Cancer Res. 2013; 73:1733–1741.
29. Biswas SK, Mantovani A. Macrophage plasticity and interaction with lymphocyte subsets: cancer as a paradigm. Nat Immunol. 2010; 11:889–896.
30. ten Hagen TL, van Vianen W, Savelkoul HF, Heremans H, Buurman WA, Bakker-Woudenberg IA. Involvement of T cells in enhanced resistance to Klebsiella pneumoniae septicemia in mice treated with liposome-encapsulated muramyl tripeptide phosphatidylethanolamine or gamma interferon. Infect Immun. 1998; 66:1962–1977.
31. Meyers PA, Schwartz CL, Krailo MD, Healey JH, Bernstein ML, Betcher D, Ferguson WS, Gebhardt MC, Goorin AM, Harris M, Kleinerman E, Link MP, Nadel H, et al. Osteosarcoma: the addition of muramyl tripeptide to chemotherapy improves overall survival – a report from the Children’s Oncology Group. J Clin Oncol. 2008; 26:633–663.