
INTRODUCTION
Metformin is the most widely prescribed drug worldwide for the treatment of type 2 diabetes. It can reduce plasma glucose levels by enhancing insulin sensitivity, which benefits patients with a variety of insulin-resistant states, including impaired glucose tolerance, polycystic ovary syndrome, obesity, and metabolic syndrome [1, 2]. Recent evidence has suggested that metformin may have anti-cancer effects. An increasing number of experimental studies has shown that metformin can effectively inhibit cell proliferation and increase chemo-sensitivity [3, 4]. Observational studies have also found that metformin use is associated with improved survival outcomes in several cancers, including prostate, pancreatic, and colorectal cancer [5–7].
Endometrial cancer is the most common cancer of the female reproductive tract in the developed countries [8]. Given that patients with advanced-stage or recurrent endometrial cancer present with a poor prognosis, it is imperative to investigate the potential factors that are related with survival outcomes in the disease. Obesity, diabetes and insulin resistance have been shown to facilitate the progression of endometrial cancer, and to be strongly associated with a poor prognosis [9, 10]. Experimental studies have demonstrated that metformin has an anti-tumorigenic potential in endometrial cancer cell lines via inhibiting cell growth and decreasing invasion and metastasis [11, 12]. Recently, several studies have tried to evaluate the effects of metformin use on survival outcomes in endometrial cancer; however, their findings were inconsistent. Some studies have shown that metformin use may be associated with improved survival in endometrial cancer [13–15], whereas others have not shown this beneficial effect [16, 17].
To better understand this issue, we carried out a systematic review and meta-analysis of the existing studies that investigated the association between metformin use and survival outcomes in patients with endometrial cancer.
RESULTS
Study selection
After screening 753 reports and conference abstracts, seven full publications and eight conference abstracts were assessed for eligibility. Of these, four records were excluded due to having no available data [18–21], and two were excluded for using overlapped data [22, 23]. Finally, six full publications and three conference abstracts were deemed to meet the eligibility criteria, and were included in the systematic review [13–17, 24–27]. A flow diagram describing study selection is shown in Figure 1.
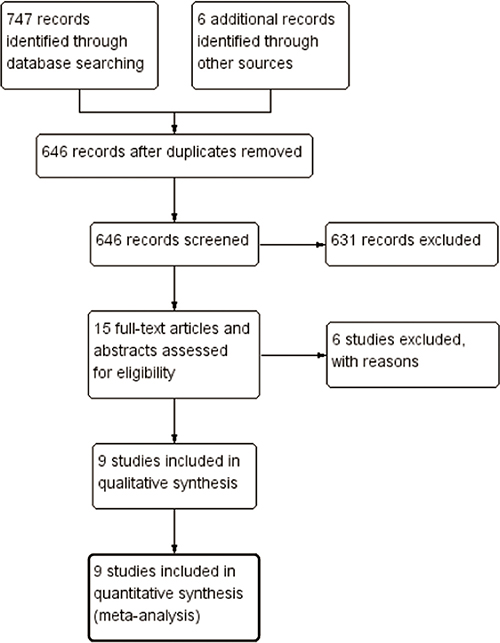
Figure 1: Study flow diagram.
Description of studies
A summary of the main characteristics of the included studies is shown in Table 1. All of the included studies were retrospective cohort studies, involving a total of 2,016 patients with endometrial cancer. The nine studies included in the systematic review were published between 2012 and 2016. Of these, seven studies were performed in the United States [13–16, 24–26], one in Poland [17], and one in Austria [27]. Six studies [14–16, 24–26] provided adjusted hazard ratio (HR) estimates, and one [17] presented a crude HR estimate in univariate analysis. Two studies [13, 27] did not provide the HRs and 95% confidence intervals (CIs), the crude HR estimates were calculated from the corresponding Kaplan-Meier curves. The Newcastle–Ottawa scale (NOS) values for the included cohort studies are shown in Table 1. All six studies were considered to be of high-quality: four studies [15, 16, 25, 26] were awarded nine stars, and two studies [17, 27] were awarded seven stars.
Table 1: Characteristics of included studies
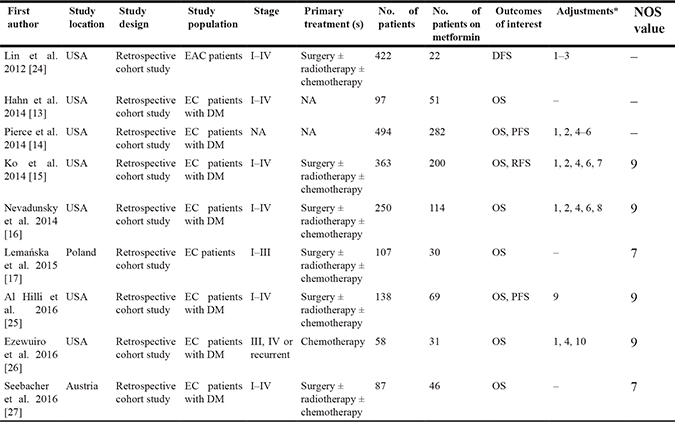
Abbreviations: EAC, endometrioid adenocarcinoma; EC, endometrial cancer; DM, diabetes mellitus; DFS, disease-free survival; OS, overall survival; PFS, progression-free survival; RFS, recurrence-free survival; NOS, Newcastle-Ottawa scale.
* 1, stage; 2, grade; 3, lymphovascular invasion; 4, age; 5, body mass index; 6, treatment; 7, histology; 8, hyperlipidemia; 9, propensity score; 10, study site.
Meta-analysis
Overall survival (OS)
Eight studies involving 1,594 individuals investigated the association between metformin use and OS [13–17, 25–27]. Four studies observed a significant inverse association between metformin use and OS [13–15, 26], while the other four studies did not [16, 17, 25, 27]. There was no substantial heterogeneity among the studies (p = 0.744; I2 = 0.0%). When we pooled the results using a fixed-effects model, metformin use was associated with significant improvements in OS (HR, 0.51; 95% CI, 0.41 to 0.64) (Figure 2).
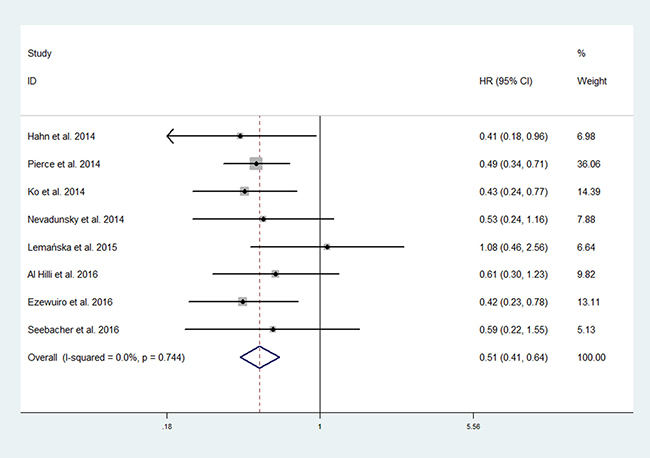
Figure 2: Forest plot of the effect of metformin use on overall survival in endometrial cancer patients.
Seven studies involving 1,487 individuals investigated the association between metformin use and OS in endometrial cancer patients with diabetes [13–16, 25–27]. There was no substantial heterogeneity among the studies (p = 0.980; I2 = 0.0%). The pooled data obtained using a fixed-effects model showed an improved OS for metformin users over non-users among endometrial cancer patients with diabetes (HR, 0.48; 95% CI, 0.38 to 0.61) (Figure 3).
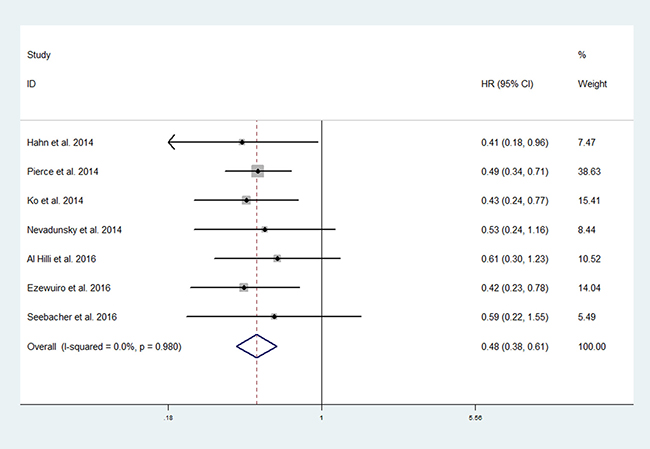
Figure 3: Forest plot of the effect of metformin use on overall survival in in endometrial cancer patients with diabetes.
To assess the stability of the results, we also conducted sensitivity analysis. In this analysis, the HR and 95% CI did not change significantly after removing any one study, confirming the stability of our results.
Progression-free survival (PFS)
Two studies involving 632 individuals explored the association between metformin use and PFS [14, 25]. There was no substantial heterogeneity among the studies (p = 0.346; I2 = 0.0%). The pooled data obtained using a fixed-effects model showed that metformin use was significantly associated with improved PFS (HR, 0.63; 95% CI, 0.46 to 0.87) (Figure 4).
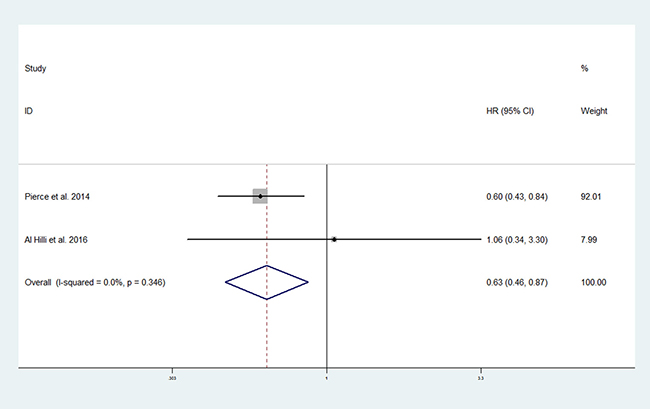
Figure 4: Forest plot of the effect of metformin use on progression-free survival in endometrial cancer patients.
Data not included in the meta-analysis
As data on either recurrence-free survival (RFS) or disease-free survival (DFS), respectively, was available in a single study, no meta-analysis was performed for these outcomes. One retrospective cohort study containing 363 diabetic endometrial cancer patients evaluated the effect of metformin use on RFS [15]. The result showed that non-metformin users was associated with decreased RFS compared to metformin users, in the unadjusted (HR: 1.7; 95% CI, 1.3 to 2.6) or adjusted model (HR: 1.8; 95% CI, 1.1 to 2.9), when adjusting for age, stage, grade, histology, and adjuvant treatment. The other retrospective cohort study containing 422 patients with endometrioid adenocarcinoma evaluated the effect of metformin use on DFS [24]. The result showed that metformin use was associated with significantly improved DFS (HR: 0.65; 95% CI, 0.43 to 0.99), after adjusting for stage, grade, and lymphovascular invasion.
DISCUSSION
With a poor prognosis associated with advanced-stage or recurrent disease, the identification of potential adjuvant agents for endometrial cancer is highly desirable. After a systematic search of published and unpublished evidence, the present systematic review identified nine cohort studies with a total of 2,016 individuals that addressed the association between metformin use and survival outcomes in endometrial cancer. Our analysis shows that metformin use is associated with improved OS and PFS in the treatment of endometrial cancer patients. Similarly, our results support the hypothesis that metformin users have longer survival as compared with metformin non-users among endometrial cancer patients with diabetes.
Experimental studies have suggested that metformin can exert anti-neoplastic effects in endometrial cancer cells. In vitro cell system analyses have demonstrated that metformin can inhibit cell proliferation, induce apoptosis, attenuate invasion and metastasis, reverse progestin resistance, and enhance chemosensitivity to cisplatin and paclitaxel [11, 12, 28–30]. The mechanisms that underlie the antineoplastic effects of metformin are incompletely understood. Directly, metformin reduces mitochondrial oxidative phosphorylation and ATP production, resulting in an increased AMP:ATP ratio, which leads to activation of the liver kinase B1 (LKB1)-dependent AMP-activated protein kinase (AMPK) pathway [31–33]. AMPK activation leads to the regulation of multiple signaling pathways that control cell proliferation, including down-regulation of the mTOR and the IGF-1/AKT pathways, and in p53-mediated cell-cycle arrest [34–36]. Indirectly, metformin reduces insulin resistance, resulting in a reduction of circulating glucose and insulin levels, which may able to inhibit tumor growth [33, 35].
Consistent with the results from laboratory studies, the present systematic review adds to the growing body of evidence supporting the concept that metformin may have therapeutic potential in endometrial cancer. Our findings are in line with the meta-analyses on the relationship between metformin use and other cancers. Similarly, they found that metformin use was associated with favorable survival outcomes for patients with kidney, pancreatic, liver, and lung cancer [37–40]. A recently published meta-analysis of six studies also found that metformin users had an improved survival over non-users among endometrial cancer patients (HR, 0.63; 95% CI, 0.45–0.87) [41].
Compared with the recently published study [41], our systematic review has several advantages. In addition to electronic databases, we also searched conference abstracts and clinical trial registers for all relevant evidence. No language restrictions were applied in our search strategy. As a result, we identified a larger number of studies as well as a larger sample size than the prior study did, which may result in more reliable findings. We considered more outcomes of interest, including OS, PFS, DFS, and RFS. Besides the consistent findings on OS, we also pooled the data on PFS and found that metformin use was significantly associated with improved PFS. Given that the observed improved OS may partly be due to the cardiovascular protective effects of metformin, the improvement in PFS identified further confirms a direct anti-neoplastic effect of metformin.
Nevertheless, our systematic review had some limitations. First, the available data was only derived from retrospective cohort studies, which may be more susceptible to bias than RCTs, due to their study design. Second, the adjusted confounders were not the same among the six studies, while no adjusted HR estimates were provided in the remaining three studies. Third, the number of included studies was small, and most of them did not report on cancer recurrence or progression outcomes, including PFS, DFS, and RFS. In addition, the dose-response analyses were not performed because most studies did not provide data on the relationship between the frequency, dose, and duration of metformin use and survival outcomes in endometrial cancer.
In conclusion, the present systematic review and meta-analysis demonstrates that metformin use is associated with improved OS and PFS in endometrial cancer patients. These findings add to the laboratory and observational data indicating that metformin may be a useful adjuvant agent in endometrial cancer. Considering the inherent biases of observational studies and the limited data, the results of this systematic review should be interpreted with caution. The full potential effect of metformin use on survival outcomes in endometrial cancer should be further rigorously accessed through randomized trials in the future.
MATERIALS AND METHODS
This systematic review and meta-analysis was prepared according to the Preferred Reporting Items for Systemic Reviews and Meta-Analyses (PRISMA) Statement [42].
Search strategy
We searched the databases of PubMed, Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL) to identify relevant studies from their inception to May 24, 2017. The detailed search strategies can be found in Supplementary Table 1. We searched the ISRCTN registry, ClinicalTrials.gov, and the World Health Organization International Clinical Trials Registry Platform (ICTRP) for relevant ongoing trials. We also searched reports from the following conferences: the Biannual Meeting of the International Gynecologic Cancer Society, the Biannual Meeting of the European Society of Gynecologic Oncology, the Annual Meeting of the American Society of Clinical Oncology, and the Annual Meeting on Women’s Cancer of the Society of Gynecologic Oncology. In addition, we scanned the references of the retrieved articles for additional eligible studies. There were no language restrictions employed in our search strategy.
Eligibility criteria
The identified potentially relevant articles were evaluated in detail to determine their eligibility. The aim was to evaluate OS, PFS, DFS, and RFS. Retrieved articles had to meet the following inclusion criteria: (1) RCTs or non-randomized studies (cohort or case-control studies) estimating the association between metformin use and survival outcomes of endometrial cancer patients; (2) full-text articles and abstracts that reported HRs and 95% CIs, or provided sufficient data to calculate these. Review articles or letters without original data, editorials, and case reports were excluded. If there were multiple publications involving the same population, the most comprehensive study was included.
Data extraction and quality assessment
Two reviewers performed data extraction independently. For each article, we collected information about the authors, publication year, study location, study population, tumor stage, sample size, outcomes of interest, HRs and 95% CIs, and variables adjusted in the analysis. The HR estimates that reflected the greatest degree of control for potential confounders were extracted whenever possible. If the HRs and 95% CIs were not available, we calculated them indirectly from Kaplan-Meier curves using published methods [43, 44]. To maintain consistency among the included studies, we extracted the HR estimates that compared metformin users with metformin non-users. When the study population was divided into three groups as non-diabetics, diabetics taking metformin, and diabetics not taking metformin, we only extracted the HR estimate that compared diabetics taking metformin and diabetics not taking metformin, in order to evaluate the effects of metformin on endometrial cancer patients with diabetes.
Since all of the included studies were cohort studies, the methodological quality was evaluated independently by two authors using the NOS [45]. The NOS uses a star system that awards from 0 to 9 stars with respect to three parameters: selection, comparability, and outcome. Since no standard criteria has been established, we considered studies that were awarded seven or more stars to be high quality studies. Any disagreements between the two authors were resolved by discussion or in consultation with a third author.
Statistical analysis
Pooled HRs with 95% CIs were used to evaluate the association of metformin use with OS and PFS of endometrial cancer patients. Heterogeneity among studies was measured using the Chi-square (χ2, or Chi2) test, and quantified using the I2 statistic. When substantial heterogeneity (p value < 0.10 or I2 > 50%) was found, pooled HRs were calculated using a random-effects model; otherwise, a fixed-effects model was applied. We planned to conduct sensitivity analyses by removing each individual study from the meta-analysis. Since the number of included studies was fewer than 10 in this meta-analysis, we did not evaluate publication bias [46, 47]. All analyses were conducted using Stata version 12.0 software (Stata Corporation, College Station, TX, USA).
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
REFERENCES
1. Hundal RS, Inzucchi SE. Metformin: new understandings, new uses. Drugs. 2003; 63:1879–1894.
2. Rajabi S, Mazloom Z, Zamani A, Tabatabaee HR. Effect of Low Glycemic Index Diet Versus Metformin on Metabolic Syndrome. Int J Endocrinol Metab. 2015; 13:e23091.
3. Pollak MN. Investigating metformin for cancer prevention and treatment: the end of the beginning. Cancer Discov. 2012; 2:778–790.
4. Kim SH, Kim SC, Ku JL. Metformin increases chemo-sensitivity via gene downregulation encoding DNA replication proteins in 5-Fu resistant colorectal cancer cells. Oncotarget. 2017; 8:56546–56557. https://doi.org/10.18632/oncotarget.17798.
5. Mayer MJ, Klotz LH, Venkateswaran V. The Effect of Metformin Use during Docetaxel Chemotherapy on Prostate Cancer Specific and Overall Survival of Diabetic Patients with Castration Resistant Prostate Cancer. J Urol. 2017; 197:1068–1075.
6. Sadeghi N, Abbruzzese JL, Yeung SC, Hassan M, Li D. Metformin use is associated with better survival of diabetic patients with pancreatic cancer. Clin Cancer Res. 2012; 18:2905–2912.
7. Garrett CR, Hassabo HM, Bhadkamkar NA, Wen S, Baladandayuthapani V, Kee BK, Eng C, Hassan MM. Survival advantage observed with the use of metformin in patients with type II diabetes and colorectal cancer. Br J Cancer. 2012; 106:1374–1378.
8. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016; 66:7–30.
9. Chia VM, Newcomb PA, Trentham-Dietz A, Hampton JM. Obesity, diabetes, and other factors in relation to survival after endometrial cancer diagnosis. Int J Gynecol Cancer. 2007; 17:441–446.
10. Zhang Y, Liu Z, Yu X, Zhang X, Lü S, Chen X, Lü B. The association between metabolic abnormality and endometrial cancer: a large case-control study in China. Gynecol Oncol. 2010; 117:41–46.
11. Tan BK, Adya R, Chen J, Lehnert H, Sant Cassia LJ, Randeva HS. Metformin treatment exerts antiinvasive and antimetastatic effects in human endometrial carcinoma cells. J Clin Endocrinol Metab. 2011; 96:808–816.
12. Cantrell LA, Zhou C, Mendivil A, Malloy KM, Gehrig PA, Bae-Jump VL. Metformin is a potent inhibitor of endometrial cancer cell proliferation--implications for a novel treatment strategy. Gynecol Oncol. 2010; 116:92–98.
13. Hahn LA, Villella JA, Chalas E, Chan KC, Jimenez EA. Metformin use is associated with improved survival in women with endometrial cancer. Gynecol Oncol. 2014; 133:159.
14. Pierce SR, Doll KM, Davidson B, Lee C, Ko EM, Snavely AC, Gehrig PA, Secord AA, Havrilesky LJ, Bae-Jump VL. Endometrial cancer outcomes in diabetic women treated with metformin, statins, and aspirin. Gynecol Oncol. 2014; 133:43.
15. Ko EM, Walter P, Jackson A, Clark L, Franasiak J, Bolac C, Havrilesky LJ, Secord AA, Moore DT, Gehrig PA, Bae-Jump V. Metformin is associated with improved survival in endometrial cancer. Gynecol Oncol. 2014; 132:438–442.
16. Nevadunsky NS, Van Arsdale A, Strickler HD, Moadel A, Kaur G, Frimer M, Conroy E, Goldberg GL, Einstein MH. Metformin use and endometrial cancer survival. Gynecol Oncol. 2014; 132:236–240.
17. Lemańska A, Zaborowski M, Spaczyński M, Nowak-Markwitz E. Do endometrial cancer patients benefit from metformin intake? Ginekol Pol. 2015; 86:419–423.
18. Woods C, Radivoyevitch T, Manochakian R, Resnick K, Klopp A, Kunos C. Impact of metformin use in diabetic women receiving endometrial cancer treatment. Int J Gynecol Cancer. 2012; 22:E1155.
19. Burnett AF, Stone RL, Hall C. The use of metformin in obese women with endometrial cancer may reduce the risk of cancer recurrence: A retrospective review. Gynecol Oncol. 2014; 133:170–171.
20. Tierney C, Miller C, Holcomb K, Wu Y, Raj S, Marshall A, Caputo TA, Gupta D. Effect of statins and metformin on survival in epithelial ovarian cancer. J Clin Oncol. 2015; 33.
21. Hall C, Stone RL, Gehlot A, Zorn KK, Burnett AF. Use of Metformin in Obese Women With Type I Endometrial Cancer Is Associated With a Reduced Incidence of Cancer Recurrence. Int J Gynecol Cancer. 2016; 26:313–317.
22. Ko E, Paige W, Clark L, Jackson A, Franasiak J, Havrilesky L, Alvarez-Secord A, Gehrig P, Bae-Jump V. Metformin reduces recurrence and improves survival in endometrial cancers. Gynecol Oncol. 2013; 130:e83.
23. Nevadunsky N, VanArsdale A, Kaur G, Frimer M, Conroy E, Einstein M, Goldberg G. Use of metformin is associated with improved endometrial cancer survival. Gynecol Oncol. 2013; 130:e74-e75.
24. Lin L, Bahng A, Rubin S, Chu C. Metformin use is associated with improved disease free survival in patients with endometrioid adenocarcinoma. Int J Gynecol Cancer. 2012; 22:E232.
25. Al Hilli MM, Bakkum-Gamez JN, Mariani A, Cliby WA, Mc Gree ME, Weaver AL, Dowdy SC, Podratz KC. The effect of diabetes and metformin on clinical outcomes is negligible in risk-adjusted endometrial cancer cohorts. Gynecol Oncol. 2016; 140:270–276.
26. Ezewuiro O, Grushko TA, Kocherginsky M, Habis M, Hurteau JA, Mills KA, Hunn J, Olopade OI, Fleming GF, Romero IL. Association of Metformin Use with Outcomes in Advanced Endometrial Cancer Treated with Chemotherapy. PLoS One. 2016; 11:e0147145.
27. Seebacher V, Bergmeister B, Grimm C, Koelbl H, Reinthaller A, Polterauer S. The prognostic role of metformin in patients with endometrial cancer: a retrospective study. Eur J Obstet Gynecol Reprod Biol. 2016; 203:291–296.
28. Zhang Z, Dong L, Sui L, Yang Y, Liu X, Yu Y, Zhu Y, Feng Y. Metformin reverses progestin resistance in endometrial cancer cells by downregulating GloI expression. Int J Gynecol Cancer. 2011; 21:213–221.
29. Hanna RK, Zhou C, Malloy KM, Sun L, Zhong Y, Gehrig PA, Bae-Jump VL. Metformin potentiates the effects of paclitaxel in endometrial cancer cells through inhibition of cell proliferation and modulation of the mTOR pathway. Gynecol Oncol. 2012; 125:458–469.
30. Dong L, Zhou Q, Zhang Z, Zhu Y, Duan T, Feng Y. Metformin sensitizes endometrial cancer cells to chemotherapy by repressing glyoxalase I expression. J Obstet Gynaecol Res. 2012; 38:1077–1085.
31. Brown KA, Samarajeewa NU, Simpson ER. Endocrine-related cancers and the role of AMPK. Mol Cell Endocrinol. 2013; 366:170–179.
32. Gallagher EJ, LeRoith D. Diabetes, cancer, and metformin: connections of metabolism and cell proliferation. Ann N Y Acad Sci. 2011; 1243:54–68.
33. Imai A, Ichigo S, Matsunami K, Takagi H, Yasuda K. Clinical benefits of metformin in gynecologic oncology. Oncol Lett. 2015; 10:577–582.
34. Pollak MN. Investigating metformin for cancer prevention and treatment: the end of the beginning. Cancer Discov. 2012; 2:778–790.
35. Stine JE, Bae-Jump V. Metformin and gynecologic cancers. Obstet Gynecol Surv. 2014; 69:477–489.
36. Pierotti MA, Berrino F, Gariboldi M, Melani C, Mogavero A, Negri T, Pasanisi P, Pilotti S. Targeting metabolism for cancer treatment and prevention: metformin, an old drug with multi-faceted effects. Oncogene. 2013; 32:1475–1487.
37. Li Y, Hu L, Xia Q, Yuan Y, Mi Y. The impact of metformin use on survival in kidney cancer patients with diabetes: a meta-analysis. Int Urol Nephrol. 2017; 49:975–981.
38. Zhou PT, Li B, Liu FR, Zhang MC, Wang Q, Li YY, Xu C, Liu YH, Yao Y, Li D. Metformin is associated with survival benefit in pancreatic cancer patients with diabetes: a systematic review and meta-analysis. Oncotarget. 2017; 8:25242–25250. https://doi.org/10.18632/oncotarget.15692.
39. Ma SJ, Zheng YX, Zhou PC, Xiao YN, Tan HZ. Metformin use improves survival of diabetic liver cancer patients: systematic review and meta-analysis. Oncotarget. 2016; 7:66202–66211. https://doi.org/10.18632/oncotarget.11033.
40. Wan G, Yu X, Chen P, Wang X, Pan D, Wang X, Li L, Cai X, Cao F. Metformin therapy associated with survival benefit in lung cancer patients with diabetes. Oncotarget. 2016; 7:35437–35445. https://doi.org/10.18632/oncotarget.8881.
41. Tang YL, Zhu LY, Li Y, Yu J, Wang J, Zeng XX, Hu KX, Liu JY, Xu JX. Metformin Use Is Associated with Reduced Incidence and Improved Survival of Endometrial Cancer: A Meta-Analysis. Biomed Res Int. 2017; 2017:5905384.
42. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010; 8:336–341.
43. Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat Med. 1998; 17:2815–2834.
44. Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials. 2007; 8:16.
45. Wells GA, Shea B, O’ Connell D, Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. [Accessed 28 May 2017].
46. Lau J, Ioannidis JP, Terrin N, Schmid CH, Olkin I. The case of the misleading funnel plot. BMJ. 2006; 333:597–600.
47. Sterne JA, Sutton AJ, Ioannidis JP, Terrin N, Jones DR, Lau J, Carpenter J, Rücker G, Harbord RM, Schmid CH, Tetzlaff J, Deeks JJ, Peters J, et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ. 2011; 343:d4002.