
INTRODUCTION
Multiple Myeloma (MM) is a malignant plasma cell disease which leads to the death of around 63 000 patients worldwide each year. [1] Despite major progress in MM treatment [2] it still remains an incurable disease.
Knowledge about the etiology of MM is still fragmentary. Overweight and obesity has a high prevalence in the western population with the tendency to rise. [3] Obesity and excessive body fat is a risk factor for cardiovascular disease, type 2 diabetes [4], and the occurrence of malignant tumors. [5–7] For MM, studies have shown that excessive body weight, measured mainly by the body mass index (BMI), is a risk factor for incidence and mortality. [8, 9]
Current disease-specific prognostic factors, like cytogenetic abnormalities [10] and the International Staging System (ISS) [11] play a major role in the course of MM. [12, 13] Compared to disease-specific prognostic factors, such as ISS and cytogenetics, also host-specific factors, such as male sex, age, black race and prior history of Monoclonal Gammopathy of Undetermined Significance influence outcome of MM patients. Among these host-specific risk factors, obesity and body fat composition would be a modifiable variable but have not been studied in symptomatic MM patients yet. This stresses the importance of further studies concerning the interactions of obesity and MM.
Whole-body low-dose computed tomography (WBLDCT) is a cornerstone in the initial work-up for newly diagnosed MM patients, since it has the highest sensitivity to detect osteolytic bone lesions. [14] Furthermore, it offers the opportunity to image and quantify the extent of visceral and subcutaneous adipose tissue as a side product.
In this study, we correlated for the first time body fat composition as assessed by WBLDCT with factors of disease activity, adverse events and treatment response in newly diagnosed MM patients enrolled in the prospective, multicenter German-Speaking Myeloma Multicenter Group (GMMG) MM-5 trial.
RESULTS
Disease activity
No correlation of parameters of body fat composition and established factors for disease activity (monoclonal protein, LDH and bone marrow plasma cells) were found.
Regarding ISS stages, a reciprocal correlation was found with the abdominal TAT (p=0.048, mean for ISS stage I = 341.55 cm2 and for ISS stage III = 278.6 cm2) and SAT (p=0.036, mean for ISS stage I = 199.46 cm2 and for ISS stage III = 164.8 cm2), visualized in Figure 1.
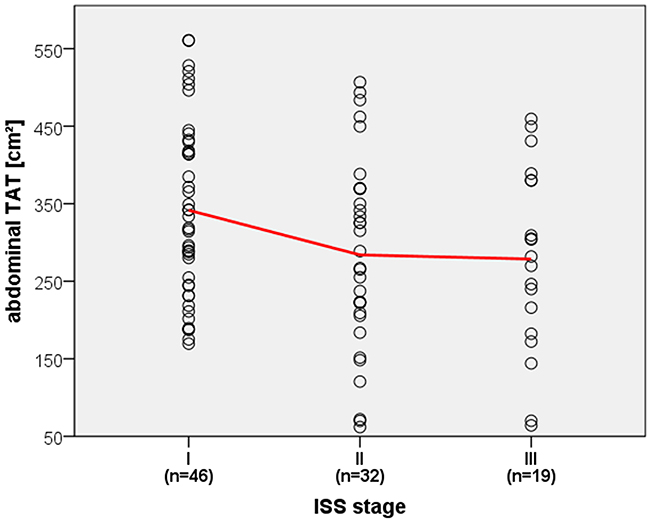
Figure 1: Correlation of ISS stage and abdominal TAT. Dotplot displaying reciprocal correlation of ISS stages and abdominal TAT with linear interpolation line highlighted in red.
No association could be found between the occurrence of CRAB criteria and body composition. However, baseline hemoglobin levels correlated significantly with abdominal TAT (p=0.008, r=0.27) and VAT (p=0.001, r=0.33) as well as pelvic VAT (p=0.006, r=0.28). Furthermore, a significant correlation was found between the occurrence of osteopenia and abdominal TAT (p=0.009) and SAT (p=0.021) as well as pelvic TAT (p=0.002), VAT (p=0.024) and SAT (p=0.006) and thigh TAT (p=0.01), displayed further in Figure 2.
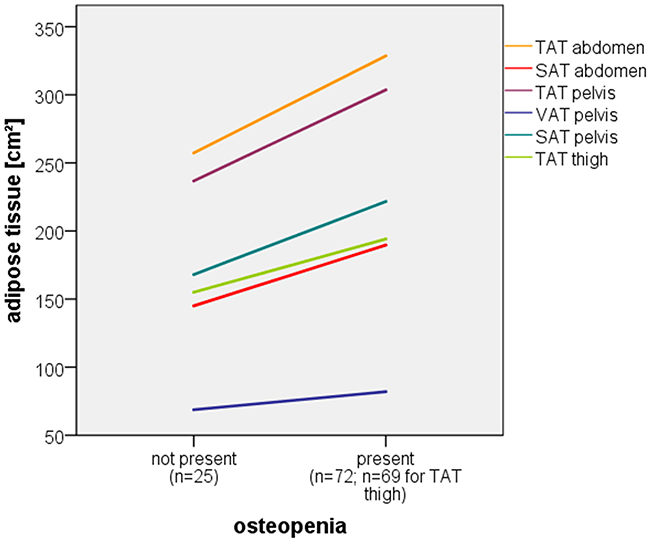
Figure 2: Correlation of osteopenia and multiple adipose tissue compartments. Line graph displaying significant correlation of osteopenia and multiple adipose tissue compartments (linear interpolation lines of mean adipose tissue values).
Adverse cytogenetics
A reciprocal correlation was observed between adverse cytogenetics and VAT of the abdomen and pelvis. The explored high risk cytogenetics consist of t(4;14) (p=0.038 for abdomen and p=0.042 for pelvis) and gain 1q21 (p=0.009 and p=0.021, respectively). Additionally TAT of the abdomen was significantly decreased under presence of t(4;14)(p=0.046). VAT of the abdomen was significantly decreased under presence of Del 13q14 (p=0.036). Del 17p13 was identified but due to the low number of positive patients (n=6/97) it was not investigated. Table 1 summarizes analysis of body compostion and cytogenetic abnormalities.
Table 1: Single factor analysis of variance (ANOVA) of mean visceral adipose tissue (VAT) values of the abdomen (abd.) and pelvis (pel.) subject to the presence of baseline cytogenetic abnormalities (CA). *=significant (p<0.05)
|
|
|
Absent CA (n) |
Present CA (n) |
P value |
|---|---|---|---|---|
|
t (4;14) |
Abd. VAT [cm2] |
137.12 (77) |
98.94 (14) |
0.038* |
|
Pel. VAT [cm2] |
80.64 (77) |
65.34 (14) |
0.042* |
|
|
gain 1q21 |
Abd. VAT [cm2] |
147.42 (54) |
110.35 (29) |
0.009* |
|
Pel. VAT [cm2] |
84.33 (54) |
70.81 (29) |
0.021* |
|
|
del 13q14 |
Abd. VAT [cm2] |
143.31 (53) |
114.65 (37) |
0.036* |
|
Pel. VAT [cm2] |
82.81 (53) |
72.14 (37) |
0.056 |
Adverse events
Analysis of adipose tissue parameters and adverse events, consisting of infection (n=29/97) and leucopenia (n=31/97), showed no significant correlation. Thrombocytopenia and thromboembolism were documented but due to the low number of affected patients (n=7/97; n=3/97, respectively) they were not statistically evaluated.
Treatment response
42 patients achieved a VGPR or better and 55 patients showed a PR or worse. Treatment response was negatively correlated to VAT of the abdomen (p=0.03) and pelvis (p=0.035). Responders thus had a lower mean VAT of the abdomen (116.17 cm2) and pelvis (72.36 cm2) than non-responders (144.22 cm2 and 83.3 cm2, respectively; Figure 3). Other adipose tissue parameters did not correlate significantly.
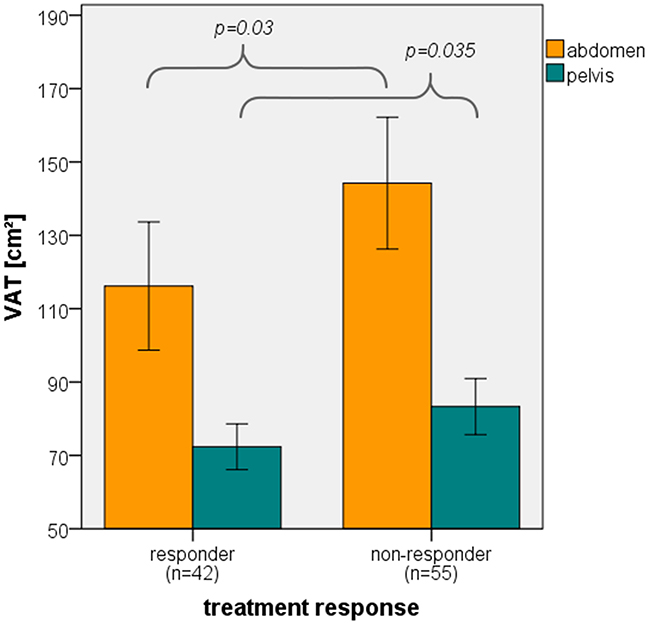
Figure 3: Correlation of treatment response and VAT. Bar graph displaying significant correlation (ANOVA) of VAT of the abdomen and pelvis and treatment response. Error bars represent 95% confidence interval.
In the multivariate analysis, the only fat parameter remaining in the model after backward selection was the abdominal VAT. It showed a significant effect on treatment response (p=0.034) even if the effect was adjusted for revised ISS and treatment. Important to note is that the results of a variable selection have to be interpreted with care as the model is somewhat optimized for the underlying data set. However, in the bootstrap analysis, abdominal visceral adipose tissue was selected in more than 40% of the bootstrap replicates such that further investigations seem well-founded.
Neither the revised ISS nor the treatment showed a significant effect on the response to treatment in the multivariate model.
Body mass index
In contrast to parameters of body fat composition, the BMI did not show a significant association with ISS (p=0.22), osteopenia (p=0.128), del13q14 (p=0.518), gain1q21 (p=0.872), t(4;14)(p=0.354) and treatment response (p=0.222). However, BMI was correlated positively with baseline hemoglobin levels (p=0.015).
DISCUSSION
With the current study we show for the first time that excessive visceral adipose tissue is associated with inferior response to a bortezomib-based induction therapy in patients with newly diagnosed, symptomatic multiple myeloma. We furthermore observed a negative correlation between visceral adipose tissue and the presence of ISS stage III and high risk cytogenetics abnormalities.
Patients with high amounts of VAT of the abdomen and pelvis showed a significantly worse treatment response, statistically independent of revised ISS stage and treatment arm. Of course, these findings need to be further investigated in future studies. For example, the development of weight gain or loss over time relating to the course of disease and therapy should be evaluated. In addition, obesity is strongly associated with multiple comorbidities commonly summarized in the context of metabolic syndrome which need to be taken into account separately in order to understand more thoroughly the interaction of these diverse variables. Further influences which could be relevant in this context, chemotherapy dosing, metabolism of body fat and its interaction with drugs as well as the influence of the immune system might be considered as well. Chemotherapy dosing is mostly calculated by the body surface area and thus, obese patients receive a lower dose of chemotherapy according to their body weight than a normal weighing patient. Furthermore, it is not clear what role the metabolism of body fat especially the abdominal VAT plays in the context of pharmacodynamics and pharmacokinetics. The proteasome inhibitor bortezomib for instance decreases MM related inflammation amongst others through inhibition of NF-κB and interaction with inflammation cytokines such as tumor necrosis factor or interleukin-6. [24, 25] Other studies have shown that adipose tissue releases proinflammatory cytokines such as the above, especially the metabolically highly active visceral compartment. [26, 27] These findings could be a plausible explanation and suggest an interference of visceral adipose tissue with the mode of action of bortezomib. Since bortezomib, included in both treatment regimens in the MM5 trial, can be applied subcutaneously, these influences are not trivial. However, recent studies in relapsed and newly diagnosed MM demonstrated that higher baseline BMI does not hamper the effect of subcutaneous bortezomib. [16, 28] Since we demonstrate with our current study that VAT might have a negative impact on treatment response, further studies are warranted examining body composition rather than BMI alone.
For all analysed high risk cytogenetic abnormalities and ISS III, a reciprocal correlation was observed. Patients with high risk cytogenetic abnormalities t(4;14) and gain1q21 as well as patients with ISS III had less adipose tissue in our analysis. Weight loss is often a first clinical “B-symptom” of B-cell lymphomas and associated with poor outcome. [29, 30] Factors produced by tumor and host cells causing lipolysis include tumor necrosis factor and interleukin 6. [31] Especially, the expression of pro-inflammatory molecules like interleukin 6 has been linked to poor survival in MM, suggesting a link between more aggressive disease and loss of adipose tissue. [32]. Another cytokine associated with progression and survival in MM as well as tumor-induced cachexia is the B-cell Activating Factor (BAFF). [33] Interestingly, BAFF expression has also been associated with proliferation and disease stage according to ISS, providing a link between disease biology weight loss. [34]
Besides the observed link between body compos-ition, the presence of cytogenetic abnormalities and treatment response, we observed a correlation of VAT with baseline hemoglobin levels. Studies have shown that men and women exhibit a different distribution of body fat. [35] While main body fat of women is located in the subcutaneous gluteofemoral area, men mainly accumulate body fat in the visceral abdomen, as shown for our patients in Figure 4. Men are known to have higher average hemoglobin levels. [36] Bringing those two facts together suggests, that the observed correlation between VAT and hemoglobin is merely due to a third variable, the male sex, in which both parameters are physiologically higher and thus seem to correlate.
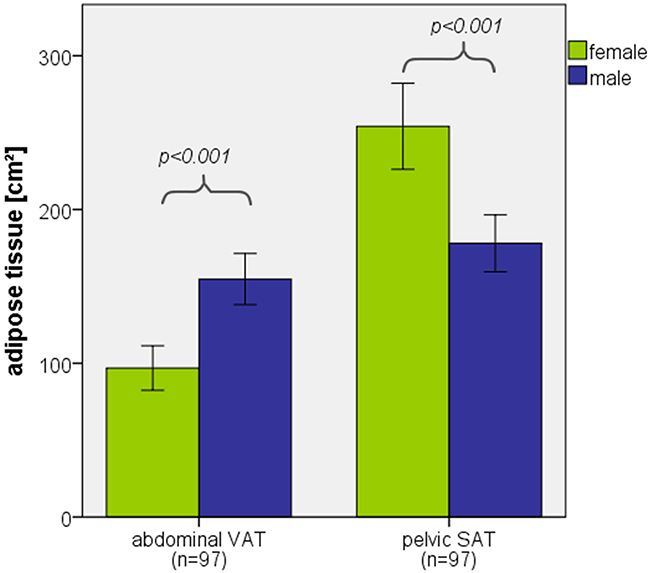
Figure 4: Distribution of adipose tissue among female and male sex. Bar graph displaying significant difference (ANOVA) of abdominal VAT and pelvic SAT distribution among female and male sex. Error bars represent 95% confidence interval.
We furthermore assume that the significant correlation between osteopenia and multiple adipose tissue parameters is rather a metabolic phenomenom than MM-related. Studies have shown that VAT, independent of MM, is a negative predictive factor for bone microarchitecture and mechanical properties in obese men. [37]
In our study, the BMI did not correlate with the treatment response and multiple other clinical and laboratory parameters, which showed a significant correlation for the WBLDCT based adipose tissue measurement. This underlines the superiority of the WBLDCT based adipose tissue measurements in comparison with the conventional measuring of weight and height for BMI calculation. Since low dose WBLDCT is a standardized staging examination for newly diagnosed MM patients, no additional examination needs to be performed for adipose tissue measurements and thus does not display additional exposure to radiation exclusively for these measurements. [38, 39] For daily clinical practice, even the measurement of one slice, preferably at the level of L3/L4, is sufficient for valid information. [40]
Furthermore, obesity is a modifiable potential predictive factor, as compared to ISS and cytogenetics. Life style changes, as a first non-invasive therapy with no major side effects and engaging in regular physical activity might have a positive effect, especially on bone health in MM patients.
In summary, we demonstrate for the first time a link between body fat composition and treatment response in patients with newly diagnosed MM. Standarized WBLDCT based adipose tissue measurement at the start of therapy might have prognostic implications and should therefore be investigated in future studies.
MATERIALS AND METHODS
Patients
In the GMMG MM5 trial, a prospective, randomized, open-label phase III trial (EudraCT n. 2010-019173-16), two regimens of bortezomib based induction therapy and lenalidomide consolidation followed by lenalidomide maintenance treatment are evaluated. [15] The therapy protocol is depicted more detailed in Figure 5. Patients with newly diagnosed, symptomatic, previously untreated MM were enrolled in 31 transplantation centers and 75 associated trial sites throughout Germany. The MM5 trial is being performed in accordance with the Declaration of Helsinki and the European Clinical Trial Directive (2005) and was approved by the local ethics committees of all participating institutions. [16] The trial has completed its recruitment and patients are in follow-up.
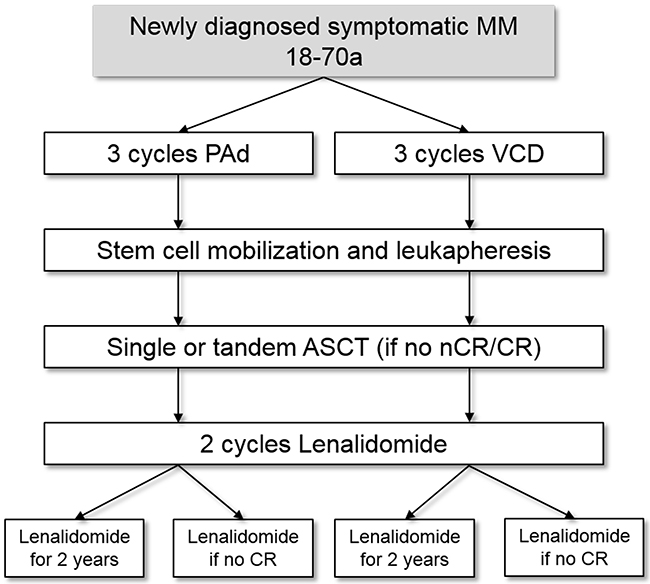
Figure 5: Treatment protocol of the GMMG MM5 study. Flow Chart of the GMMG MM5 study. Patients were randomized to four treatment arms with either PAd (2 arms) or VCD (2 arms) induction therapy and lenalidomide maintenance therapy either for 2 years or until complete response was achieved. PAd: bortezomib-adriamycin-dexamethasone; VCD: bortezomib-cyclophosphamide-dexamethasone; ASCT: autologous stem cell transplantation; CR: complete response; nCR: near complete response.
In this retrospective study, a subgroup of 108 patients enrolled at our trial site in the MM5 trial, who received WBLDCT before 3 cycles induction therapy (VCD [bortezomib, cyclophosphamide, dexamethasone] or PAd [bortezomib, adriamycin, dexamethasone]) as part of the standardized staging examination, were included. WBLDCTs of 97 patients were technically viable for the planned analysis. Exclusion criteria included incomplete image data set (n=10) or patient outside of the field of view (n=1). Data on disease activity, adverse cytogenetics, adverse events and treatment response were captured in the context of the MM5 trial. Patients´ characteristics are summarized in Table 2.
Table 2: Baseline characteristics of included patients
|
Sex |
|
|---|---|
|
Female [n] |
38 (39%) |
|
Underweight (<18,5 kg/m2) |
1 |
|
Normal weight (18,5-24,9 kg/m2) |
19 |
|
Overweight (25-29,9 kg/m2) |
10 |
|
Obese (≥30 kg/m2) |
8 |
|
Male [n] |
59 (61%) |
|
Underweight (<18,5 kg/m2) |
0 |
|
Normal weight (18,5-24,9 kg/m2) |
21 |
|
Overweight (25-29,9 kg/m2) |
28 |
|
Obese (≥30 kg/m2) |
10 |
|
Demographics (median (range)) |
|
|
Age [a] |
59 (33-70) |
|
BMI [kg/m2] |
26 (18.4-39.8) |
|
Height [cm] |
172 (155-197) |
|
Weight [kg] |
77 (49-121) |
|
Treatments |
|
|
PAd [n] |
44 (45%) |
|
VCD [n] |
53 (55%) |
|
Disease activity (median (range)) |
|
|
Monoclonal protein [g/l] |
42 (4-102.9) |
|
LDH [U/l] |
192 (105-415) |
|
Plasma cells [%] |
40 (1-95) |
|
ISS (I, II, III) [n] |
46 (47%), 32 (33%), 19 (20%) |
|
CRAB criteria (median (range)) |
|
|
Calcium [mmol/l] |
2.37 (1.93-3.68) |
|
Creatinine [mg/dl] |
0.93 (0.54-11.04) |
|
Hemoglobin [g/dl] |
11 (7.9-16.3) |
|
Osteopenia (present) [n] |
72 (74%) |
|
Osteolysis (present) [n] |
80 (82%) |
|
Fracture (present) [n] |
38 (39%) |
|
Adverse cytogenetics |
|
|
T(4;14) (present) [n] |
14/91 (15%) |
|
Del 17p13 (present) [n] |
5/92 (5%) |
|
Gain 1q21 (present) [n] |
29/83 (35%) |
|
Del 13q14 (present) [n] |
37/90 (41%) |
Protocol for body fat composition measurement
WBLDCTs were provided through the Picture Archiving and Communication System (PACS, Centricity® 4.1, GE Healthcare, Barrington, IL, USA) of the Department of Diagnostic and Interventional Radiology of the University of Heidelberg (DDIR, n=74) and the German Cancer Research Center Heidelberg (DKFZ, n=21), Germany. External institutions provided 4 WBLDCTs. A low dose protocol was used with a median slice thickness of 3 mm (min: 1 mm; max: 5 mm) and no contrast media was administered. The measurements were performed using the “CT volume tool” of the “SyngoVia” software (Siemens Healthcare GmbH, Munich, Germany).
In order to define adipose tissue compartments, regions of interests (ROIs) were drawn manually into images of the most cranial and caudal slice. ROIs in remaining slices were generated by the software. Each ROI was then visually inspected and adjusted manually, if necessary. An attenuation limit of -190 to -30 Hounsfield Units (HU) was assumed to represent adipose tissue. [17–19]
Measurements were divided into the three compartments: Abdomen, pelvis and thigh. Abdomen was measured from the intervertebral space between the 11th and 12th thoracic vertebral body (TH11 and TH12) to the intervertebral space between the 5th lumbar vertebral body (L5) and the 1st sacral vertebral body (S1). Pelvis was defined from the intervertebral space between L5 and S1 to the top of the symphysis. The thigh compartment was measured from the top of the symphysis to the top of the patella.
The total adipose tissue (TAT) measurements in the abdomen and pelvis were further categorized into the visceral (VAT) and subcutaneous adipose tissue (SAT), whereas in the thigh compartment only the TAT was determined.
The visceral compartment is circumscribed by abdominal wall muscles. In the dorsal direction, the compartment was restricted by bony structures of the spine and, further caudal, by the pelvic structure. For the pelvic measurements, the intrapelvic part of the piriformis muscle and the psoas muscle cranial of its crossing with the inguinal ligament were included. Figure 6 illustrates these measurements by means of sample CT images.
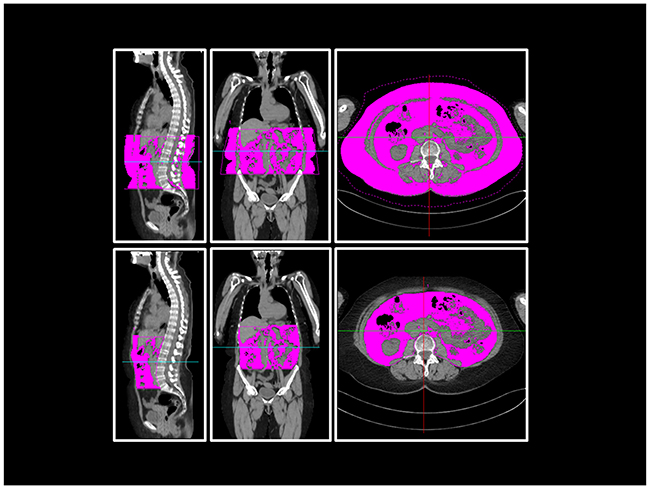
Figure 6: Body fat composition measurement in WBLDCT. Example sagittal, coronal and axial views at the level of L3 of WBLDCT of a patient. Purple-coloured areas represent the measured total (above) and visceral (below) adipose tissue of the abdominal compartment.
For further calculations, the measured adipose tissue volume was divided by the individual height of the equivalent compartment in order to be comparable among each other. Thus, the calculations were performed with a virtual area (values in square centimeter) representing the measured adipose tissue in the entire compartment.
Moreover, the BMI at time of the WBLDCT was gathered in order to investigate its correlation with disease activity, adverse cytogenetics, adverse events and treatment response.
The investigator was blinded with regard to patients´ disease activity, adverse cytogenetics, adverse events and treatment response.
Disease activity and adverse cytogenetics
Monoclonal protein, bone marrow plasma cells, lactate dehydrogenase (LDH), ISS and CRAB-criteria [20] (calcium, creatinine, hemoglobin and osteopenia/osteolyses/fractures) were chosen to represent the current disease activity. Bone related disease activity for the CRAB-criteria were provided by the radiological reports from the WBLDCTs. In order to detect cytogenetic abnormalities, Interphase fluorescence in situ hybridization analysis was performed on CD138-purified plasma cells. Deletion 17p13, translocation t(4;14) and gain 1q21 >3 copies were defined as adverse cytogenetics. [21] Deletion 13q14 was additionally evaluated in this study.
Adverse events and treatment response
Adverse events were graded using the CTCAE catalogue, version 4.0, of the National Institutes of Health (NIH). [22] Adverse events analyzed in this study were infections (CTC grade 2 or greater), leukopenia (CTC grade 3 or greater), thrombocytopenia (CTC grade 3 or greater) and thromboembolism (CTC grade 2 or greater). Treatment response was assessed according to the International Myeloma Working Group (IMWG) Uniform Response Criteria, modified to include near complete response. [23] Patients achieving at least a very good partial response (VGPR) after induction therapy were classified as responders.
Statistical analysis
In a first step, univariate analyses were used to get a first impression of the effects of the fat parameters on treatment response and to identify possible confounders. The parameters were divided into continuous variables (monoclonal protein, LDH, plasma cells, calcium, creatinine, hemoglobin, BMI) and categorical variables (ISS, osteopenia, osteolysis, fracture, del 17p13, t(4;14), gain 1q21, del 13q14, treatment response, infection, leukopenia, thrombocytopenia, thromboembolism) for the statistical analysis. The continuous variables were analysed using the Pearson correlation or the Spearman correlation respectively in case of non-normally distributed variables. The single factor analysis of variance (univariate ANOVA or Kruskal-Wallis test) was used for categorical variables. P values lower than 0.05 were considered statistically significant. Due to the explorative character of these investigations, correction for multiple testing was omitted.
To further investigate the association between the body fat composition and the treatment response in the presence of confounders and to be able to account for the correlation structure between the fat parameters, a multivariate logistic regression model was fitted. Revised ISS (combination of ISS, cytogenetics and LDH) [13] and treatment arm (VCD/PAD) were included into the model as relevant prognostic factors. Fat parameters (VAT and SAT of the abdomen and pelvis and TAT of the thigh compartment) with an additional effect on the response to treatment even in the presence of confounders were determined using backward selection. That is, the fat parameters were excluded from the full model in a stepwise fashion until the p-values for all remaining fat parameters in the model are less than 0.1. Instead of the usual significance level of 0.05, the cut-off of 0.1 was chosen to overcome the lack of power to detect a true predictor due to small sample size.
For validation of the variable selection method, the stability of the selection algorithm was investigated by means of bootstrapping. Therefore, 500 bootstrap samples of 94 patients each (number of complete observations for the multivariate model) were drawn with replacement from the original data set and for each sample, the variable selection method was conducted. Selection frequencies for each of the fat parameters were estimated by the proportion of bootstrap replicates in which the corresponding variable was selected.
All analyses were performed with software R, Version 3.0.2 (R Foundation, Vienna, Austria) and SPSS (IBM, Armonk, USA). The multivariate analysis was performed with R, Version 3.3.1.
Abbreviations
BAFF, B-cell Acitivating Factor
BMI, body mass index
GMMG, German-Speaking Myeloma Multicenter Group
HU, Hounsfield Units
IMWG, International Myeloma Working Group
ISS, International Staging System
LDH, lactate dehydrogenase
MM, multiple myeloma
PAd, bortezomib, adriamycin, dexamethasone
ROI, region of interest
SAT, subcutaneous adipose tissue
TAT, total adipose tissue
VAT, visceral adipose tissue
VCD, bortezomib, cyclophosphamide, dexame-thasone
VGPR, very good partial response
WBLDCT, whole-body low-dose computed tomography
Author contributions
conception and design: Groß JP, Nattenmüller J, Hemmer S, Hillengass J, Merz M
acquisition of data and analysis: Groß JP, Tichy D, Krzykalla J, Goldschmidt H, Bertsch U, Hillengass J, Merz M
article drafting: Groß JP, Krzykalla J, Hillengass J, Merz M
revision and final approval: Groß JP, Nattenmüller J, Hemmer S, Tichy D, Krzykalla J, Goldschmidt H, Bertsch U, Delorme S, Kauczor HU, Hillengass J, Merz M
ACKNOWLEDGMENTS
The authors thank the investigators, the study nurses and all members of the study teams at the participating GMMG trial sites, the teams of the myeloma research laboratory, the FISH laboratory and the central laboratory at the University Hospital Heidelberg, the coordination centers for clinical trials (KKS) in Heidelberg and Leipzig, the pharmacies at the trial sites and, most importantly, the participating patients and their families.
CONFLICTS OF INTEREST
There are no conflicts of interest to declare among the authors.
FUNDING
The GMMG MM5 Trial (EudraCT n. 2010-019173-16) is supported by grants from Janssen-Cilag, Celgene, Chugai and The Binding Site. For this study, a travel grant for poster presentation from Novartis Pharma GmbH was received.
REFERENCES
1. Becker N. Epidemiology of multiple myeloma. Recent Results Cancer Res. 2011; 183: 25–35. https://doi.org/10.1007/978-3-540-85772-3_2.
2. Merz M, Hillengass J, Goldschmidt H. Meeting report of the 5th Heidelberg Myeloma Workshop: current status and developments in diagnosis and therapy of multiple myeloma. J Cancer Res Clin Oncol. 2015; 142:247-51. https://doi.org/10.1007/s00432-015-1993-3.
3. Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA. 2014; 311: 806–14. https://doi.org/10.1001/jama.2014.732.
4. Pérez Pérez A, Ybarra Muñoz J, Blay Cortés V, de Pablos Velasco P. Obesity and cardiovascular disease. Public Health Nutr. 2007; 10: 1156–63. https://doi.org/10.1017/S1368980007000651.
5. Wolin KY, Carson K, Colditz GA. Obesity and cancer. The Oncologist. 2010; 15: 556–65. https://doi.org/10.1634/theoncologist.2009-0285.
6. Murphy F, Kroll ME, Pirie K, Reeves G, Green J, Beral V. Body size in relation to incidence of subtypes of haematological malignancy in the prospective Million Women Study. Br J Cancer. 2013; 108: 2390–8. https://doi.org/10.1038/bjc.2013.159.
7. Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M. Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet Lond Engl. 2008; 371: 569–78. https://doi.org/10.1016/S0140-6736(08)60269-X.
8. Carson KR, Bates ML, Tomasson MH. The skinny on obesity and plasma cell myeloma: a review of the literature. Bone Marrow Transplant. 2014; 49: 1009–15. https://doi.org/10.1038/bmt.2014.71.
9. Wallin A, Larsson SC. Body mass index and risk of multiple myeloma: a meta-analysis of prospective studies. Eur J Cancer Oxf Engl 1990. 2011; 47: 1606–15. https://doi.org/10.1016/j.ejca.2011.01.020.
10. Rajan AM, Rajkumar SV. Interpretation of cytogenetic results in multiple myeloma for clinical practice. Blood Cancer J. 2015; 5: e365. https://doi.org/10.1038/bcj.2015.92.
11. Greipp PR, San Miguel J, Durie BGM, Crowley JJ, Barlogie B, Bladé J, Boccadoro M, Child JA, Avet-Loiseau H, Harousseau JL, Kyle RA, Lahuerta JJ, Ludwig H, et al. International staging system for multiple myeloma. J Clin Oncol. 2005; 23: 3412–20. https://doi.org/10.1200/JCO.2005.04.242.
12. Moreau P, Cavo M, Sonneveld P, Rosinol L, Attal M, Pezzi A, Goldschmidt H, Lahuerta JJ, Marit G, Palumbo A, van der Holt B, Bladé J, Petrucci MT, et al. Combination of international scoring system 3, high lactate dehydrogenase, and t(4;14) and/or del(17p) identifies patients with multiple myeloma (MM) treated with front-line autologous stem-cell transplantation at high risk of early MM progression-related death. J Clin Oncol. 2014; 32: 2173–80. https://doi.org/10.1200/JCO.2013.53.0329.
13. Palumbo A, Avet-Loiseau H, Oliva S, Lokhorst HM, Goldschmidt H, Rosinol L, Richardson P, Caltagirone S, Lahuerta JJ, Facon T, Bringhen S, Gay F, Attal M, et al. Revised international staging system for multiple myeloma: a report from international myeloma working group. J Clin Oncol. 2015; 33: 2863–9. https://doi.org/10.1200/JCO.2015.61.2267.
14. Pianko MJ, Terpos E, Roodman GD, Divgi CR, Zweegman S, Hillengass J, Lentzsch S. Whole-body low-dose computed tomography and advanced imaging techniques for multiple myeloma bone disease. Clin Cancer Res. 2014; 20: 5888–97. https://doi.org/10.1158/1078-0432.CCR-14-1692.
15. Mai EK, Bertsch U, Dürig J, Kunz C, Haenel M, Blau IW, Munder M, Jauch A, Schurich B, Hielscher T, Merz M, Huegle-Doerr B, Seckinger A, et al. Phase III trial of bortezomib, cyclophosphamide and dexamethasone (VCD) versus bortezomib, doxorubicin and dexamethasone (PAd) in newly diagnosed myeloma. Leukemia. 2015; 29: 1721–9. https://doi.org/10.1038/leu.2015.80.
16. Merz M, Salwender H, Haenel M, Mai EK, Bertsch U, Kunz C, Hielscher T, Blau IW, Scheid C, Hose D, Seckinger A, Jauch A, Hillengass J, et al. Subcutaneous versus intravenous bortezomib in two different induction therapies for newly diagnosed multiple myeloma: an interim analysis from the prospective GMMG-MM5 trial. Haematologica. 2015; 100: 964–9. https://doi.org/10.3324/haematol.2015.124347.
17. Sjöström L, Kvist H, Cederblad A, Tylén U. Determination of total adipose tissue and body fat in women by computed tomography, 40K, and tritium. Am J Physiol. 1986; 250: E736–45.
18. Yoshizumi T, Nakamura T, Yamane M, Islam AH, Menju M, Yamasaki K, Arai T, Kotani K, Funahashi T, Yamashita S, Matsuzawa Y. Abdominal fat: standardized technique for measurement at CT. Radiology. 1999; 211: 283–6. https://doi.org/10.1148/radiology.211.1.r99ap15283.
19. Nattenmueller J, Hoegenauer H, Boehm J, Scherer D, Paskow M, Gigic B, Schrotz-King P, Grenacher L, Ulrich C, Kauczor HU. CT-based compartmental quantification of adipose tissue versus body metrics in colorectal cancer patients. Eur Radiol. 2016; 26:4131-4140. https://doi.org/10.1007/s00330-016-4231-8.
20. Rajkumar SV, Dimopoulos MA, Palumbo A, Blade J, Merlini G, Mateos MV, Kumar S, Hillengass J, Kastritis E, Richardson P, Landgren O, Paiva B, Dispenzieri A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014; 15: e538–48. https://doi.org/10.1016/S1470-2045(14)70442-5.
21. Sawyer JR. The prognostic significance of cytogenetics and molecular profiling in multiple myeloma. Cancer Genet. 2011; 204: 3–12. https://doi.org/10.1016/j.cancergencyto.2010.11.002.
22. US Department of Health and Human Services; National Institutes of Health; National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE) - Version 4.0 [Internet]. 2010 [cited 2015 Dec 23]. Available from http://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_QuickReference_8.5x11.pdf
23. Durie BG, Harousseau JL, Miguel JS, Bladé J, Barlogie B, Anderson K, Gertz M, Dimopoulos M, Westin J, Sonneveld P, Ludwig H, Gahrton G, Beksac M, et al. International uniform response criteria for multiple myeloma. Leukemia. 2006; 20: 1467–73. https://doi.org/10.1038/sj.leu.2404284.
24. Nencioni A, Grünebach F, Patrone F, Ballestrero A, Brossart P. Proteasome inhibitors: antitumor effects and beyond. Leukemia. 2007; 21: 30–6. https://doi.org/10.1038/sj.leu.2404444.
25. Mitsiades N, Mitsiades CS, Poulaki V, Chauhan D, Richardson PG, Hideshima T, Munshi N, Treon SP, Anderson KC. Biologic sequelae of nuclear factor-kappaB blockade in multiple myeloma: therapeutic applications. Blood. 2002; 99: 4079–86.
26. Fontana L, Eagon JC, Trujillo ME, Scherer PE, Klein S. Visceral fat adipokine secretion is associated with systemic inflammation in obese humans. Diabetes. 2007; 56: 1010–3. https://doi.org/10.2337/db06-1656.
27. Tchernof A, Després JP. Pathophysiology of human visceral obesity: an update. Physiol Rev. 2013; 93: 359–404. https://doi.org/10.1152/physrev.00033.2011.
28. Moreau P, Pylypenko H, Grosicki S, Karamanesht I, Leleu X, Grishunina M, Rekhtman G, Masliak Z, Robak T, Shubina A, Arnulf B, Kropff M, Cavet J, et al. Subcutaneous versus intravenous administration of bortezomib in patients with relapsed multiple myeloma: a randomised, phase 3, non-inferiority study. Lancet Oncol. 2011; 12: 431–40. https://doi.org/10.1016/S1470-2045(11)70081-X.
29. International Non-Hodgkin's Lymphoma Prognostic Factors Project. A predictive model for aggressive non-Hodgkin’s lymphoma. N Engl J Med. 1993; 329: 987–94. https://doi.org/10.1056/NEJM199309303291402.
30. Ng AK, Bernardo MP, Weller E, Backstrand KH, Silver B, Marcus KC, Tarbell NJ, Friedberg J, Canellos GP, Mauch PM. Long-term survival and competing causes of death in patients with early-stage Hodgkin’s disease treated at age 50 or younger. J Clin Oncol. 2002; 20: 2101–8.
31. Ebadi M, Mazurak VC. Evidence and mechanisms of fat depletion in cancer. Nutrients. 2014; 6: 5280–97. https://doi.org/10.3390/nu6115280.
32. Bataille R, Boccadoro M, Klein B, Durie B, Pileri A. C-reactive protein and beta-2 microglobulin produce a simple and powerful myeloma staging system. Blood. 1992; 80: 733–7.
33. Rihacek M, Bienertova-Vasku J, Valik D, Sterba J, Pilatova K, Zdrazilova-Dubska L. B-cell activating factor as a cancer biomarker and its implications in cancer-related cachexia. Bio Med Res Int. 2015; 2015:792187. https://doi.org/10.1155/2015/792187.
34. Hengeveld PJ, Kersten MJ. B-cell activating factor in the pathophysiology of multiple myeloma: a target for therapy? Blood Cancer J. 2015; 5: e282. https://doi.org/10.1038/bcj.2015.3.
35. Karastergiou K, Smith SR, Greenberg AS, Fried SK. Sex differences in human adipose tissues - the biology of pear shape. Biol Sex Differ. 2012; 3: 13. https://doi.org/10.1186/2042-6410-3-13.
36. Murphy WG. The sex difference in haemoglobin levels in adults — mechanisms, causes, and consequences. Blood Rev. 2014; 28: 41–7. https://doi.org/10.1016/j.blre.2013.12.003.
37. Bredella MA, Lin E, Gerweck AV, Landa MG, Thomas BJ, Torriani M, Bouxsein ML, Miller KK. Determinants of bone microarchitecture and mechanical properties in obese men. J Clin Endocrinol Metab. 2012; 97: 4115–22. https://doi.org/10.1210/jc.2012-2246.
38. Hillengass J, Delorme S. Multiple myeloma: current recommendations for imaging. [Article in German]. Radiologe. 2012; 52: 360–5. https://doi.org/10.1007/s00117-011-2257-0.
39. Hillengass J, Landgren O. Challenges and opportunities of novel imaging techniques in monoclonal plasma cell disorders: imaging “early myeloma.” Leuk Lymphoma. 2013; 54: 1355–63. https://doi.org/10.3109/10428194.2012. 740559.
40. Irlbeck T, Massaro JM, Bamberg F, O’Donnell CJ, Hoffmann U, Fox CS. Association between single-slice measurements of visceral and abdominal subcutaneous adipose tissue with volumetric measurements: the Framingham Heart Study. Int J Obes 2005. 2010; 34: 781–7. https://doi.org/10.1038/ijo.2009.279.