
INTRODUCTION
Malignant pleural mesothelioma (PM) is a rare (incidence, 7/1.000.000/year) aggressive cancer associated with occupational exposure to asbestos that is often diagnosed at late, unresectable stages [1, 2]. Despite aggressive treatment algorithms including radiation and/or chemotherapy, the prognosis of mesothelioma has remained poor for decades, with an average survival of 9–12 months [3]. Therefore, new molecular targets for this fatal disease need to be identified.
C-X-C motif chemokine receptor 4 (CXCR4) and its ligand CXCL12 play an important role in a variety of physiological processes that rely on the recruitment and homing of stem cells, progenitor cells and immune cells. CXCR4 is over-expressed in more than 20 human tumor types, promoting tumor growth and progression, tumor invasiveness and metastasis [4]. In malignant mesothelioma, robust overexpression of CXCR4 was reported in human mesothelioma cell lines and the majority of mesothelioma tissues, respectively [5].
Recently, Wester and co-workers developed [68Ga]Pentixafor ([68Ga]CPCR4.2), a cyclic pentapeptide that enables sensitive and high-contrast imaging of human CXCR4 receptor expression in vivo [6–8] . Proof-of-concept visualization with this tracer could be demonstrated for several different hematologic and other neoplasms including leukemia, lymphoma, multiple myeloma, glioblastoma or small cell lung cancer, but also in other (inflammatory) disease conditions, such as stroke and myocardial infarction [9–15]. Interestingly, in a pilot study, the in vitro CXCR4 expression profile of solid cancers was shown to be different from the in vivo distribution as revealed by CXCR4-targeted PET imaging [16].
The aim of this pilot study was to assess the feasibility of non-invasive imaging of CXCR4 in patients with pleural mesothelioma.
RESULTS
Patients
Histopathologic diagnosis had been derived by surgical or biopsy samples in all patients. 4/6 patients suffered from epitheloid, the remaining subjects from desmoplastic/sarcomatoid and microcystic mesothelioma, respectively. All subjects presented with diseases confined to the mesothelial surfaces of the pleural cavity. No extra-pleural metastatic sites were present at the time point of imaging (Supplementary Table 1).
Surgical samples
The surgical samples available for IHC were derived from patients with epitheloid (n = 4), sarcomatoid (n = 3), and biphasic (n = 2) mesothelioma, respectively. All samples were derived from patients (8 males, 1 female) with the primary diagnosis of PM. None of them presented with extra-pleural metastases.
Image analysis
On visual image analysis of the scans, none of the six patients presented relevant focal [68Ga]Pentixafor-positive lesions (Figure 1). Only physiologic tracer distribution was recorded.
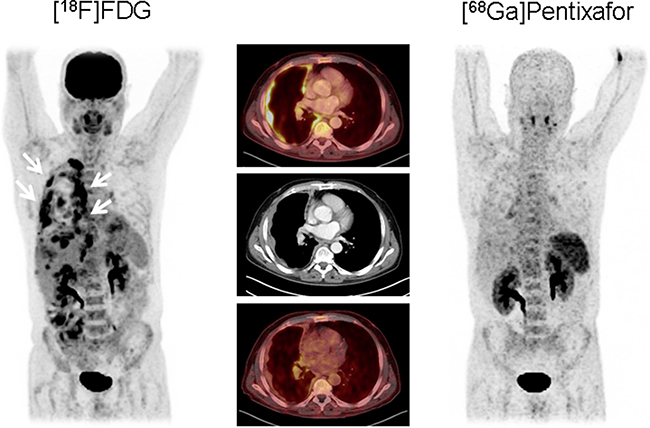
Figure 1: Example of epitheloid mesothelioma (patient #3) without relevant CXCR4 expression. Maximum intensity projections (outer columns) and transaxial slices (middle column) of [18F]FDG PET/CT (left, upper row of the middle column) and [68Ga] Pentixafor PET/CT (right, lower row of middle column) in a patient with the primary diagnosis of epitheloid mesothelioma. The multiple vital tumor lesions along the right pleura detected by [18F]FDG PET/CT (arrows) do not express CXCR4. This finding was confirmed by immunohistochemistry.
In semi-quantitative analysis, SUVmean ranged from 1.4 to 2.9 with a median of 2.5 and SUVmax from 2.3 to 4.4 with a median of 3.9, respectively. Median blood pool activity was 1.8 (range, 1.6–2.7) for SUVmean and 3.6 (range, 2.8–4.6) for SUVmax. Accordingly, tumor-to-blood pool (TBR) ratios were low in all cases with a median of 1.2 (range, 0.9–1.6) for TBRmean and 1.0 for TBRmax (range, 0.7–1.4), respectively.
In contrast, [18F]FDG-PET identified viable tumor lesions in all patients with SUVmean ranging from 5.8 to 11.3 (median, 8.3) and SUVmax from 7.8 to 18.4 (median, 11.5), respectively. With median blood pool uptake of 1.8 (SUVmean, range, 1.7 to 2.2) and 2.7 (SUVmax, range, 2.0 to 3.2), median TBRs were 4.9 (range, 2.9–5.1) for SUVmean and 5.2 (range, 2.5–5.8) for SUVmax, respectively. Results for each individual patient are mentioned in Table 1.
Table 1: Individual imaging results
No. |
Age |
Sex |
[68Ga]Pentixafor |
[18F]FDG |
||||||
|---|---|---|---|---|---|---|---|---|---|---|
SUVmean |
SUVmax |
TBRmean |
TBRmax |
SUVmean |
SUVmax |
TBRmean |
TBRmax |
|||
1 |
54 |
M |
2.3 |
4.4 |
1.3 |
1.0 |
n/a |
n/a |
n/a |
n/a |
2 |
69 |
F |
2.7 |
3.9 |
1.6 |
1.3 |
8.0 |
11.0 |
4.8 |
5.4 |
3 |
60 |
M |
1.4 |
2.3 |
0.9 |
0.7 |
8.6 |
12.0 |
5.0 |
5.0 |
4 |
78 |
M |
2.5 |
3.9 |
1.1 |
1.0 |
n/a |
n/a |
n/a |
n/a |
5 |
73 |
M |
2.9 |
3.6 |
1.1 |
0.9 |
5.8 |
7.8 |
3.0 |
2.5 |
6 |
80 |
M |
2.5 |
3.8 |
1.6 |
1.4 |
11.3 |
18.4 |
5.1 |
5.8 |
n/a = not available.
Immunohistochemistry
In all patients, imaging results could be compared to CXCR4 expression in biopsies or surgical specimens of the primary tumors assessed by immunohistochemistry. Regarding the histological evaluation of membranous CXCR4 expression, none of samples revealed specific staining for the chemokine receptor (Figure 2).
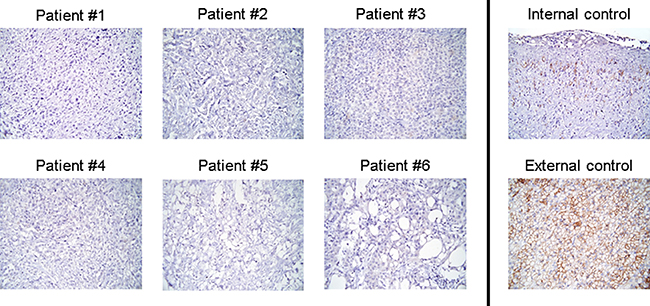
Figure 2: Individual IHC results for CXCR4. Display of the individual results of immunohistochemistry (IHC) for the six patients undergoing [68Ga]Pentixafor-PET/CT. In parallel to imaging, no significant CXCR4 expression could be demonstrated on the tumor cell surface. Vascular epithelium served as internal and adrenocortical tissue as external control. Magnification: ×400.
Nine additional surgical mesothelioma samples from patients not undergoing CXCR4-directed imaging were available for analysis. In parallel with the findings for the patients in whom imaging was performed, all samples were negative for CXCR4 expression in IHC.
DISCUSSION
This is the first report of in vivo imaging of CXCR4 expression in humans with pleural mesothelioma. Whereas a first study on malignant mesothelioma cells (derived from pleural effusions) showed an infrequent chemokine receptor expression [17], a recent report evaluating mesothelioma cell lines and biopsy samples demonstrated a robust CXCR4 receptor expression in malignant PM [5]. Strikingly, IHC for CXCR4 was principally positive in 5 of 6 human mesothelioma cell lines as well as 31/41 mesothelioma tissues. Almost 40% of patient samples demonstrated strong chemokine receptor expression as determined by IHC.
In contrast, in our cohort of PM patients and mesothelioma samples, no significant receptor expression was identified, neither by PET/CT imaging nor immunohistochemical staining. Of note, in the cases with corresponding [18F]FDG-PET/CT serving as reference, all tumor lesions exhibited intense FDG uptake (as a marker of tumor viability) with high tumor-to-background ratios. Thus, our findings are in line with a previous study reporting on a rather lower CXCR4 expression profile of solid cancers and metastases (not including mesothelioma) in vivo [16]. The reason for this obvious discrepancy to the past series is unclear. As a potential explanation, one might argue that cell lines do not fully represent in vivo disease, e.g. due to the lack of the tumor microenvironment. The differences in tissue samples might be explained by the fact that receptor surface expression of CXCR4 is a dynamic process which is influenced by a number of factors including therapeutic agents. However, in IHC analyses we did not only find no CXCR4 at the cell surface but also no evidence/indication of intracellular CXCR4 protein expression. In our small cohort, all patients were treatment-naïve at the time of both imaging and biopsy/surgery. Though Li et al. report that all patients´ samples in their study were directly obtained from surgery we cannot exclude the possibility of altered CXCR4 expression due to potential previous therapies. Future studies to further investigate therapy-induced down- and –preferably- up-regulation of CXCR4 are highly warranted.
In cell culture experiments, Li and co-workers could also demonstrate that CXCL12, the sole ligand of CXCR4, can induce proliferation in mesothelioma which can be antagonized by administration of CXCR4 inhibitors such as AMD3100 [5]. Given the high cellular expression of the chemokine receptor in vitro as well as the effects of CXCR4 inhibition, the authors concluded that CXCR4-directed therapies might prove beneficial in high-expressing tumors. Since the advent of [68Ga]Pentixafor and its therapeutic counterpart, [90Y]/[177Lu]Pentixather, theranostic concepts for CXCR4 have successfully introduced by nuclear medicine [18]. Given the high receptor expression previously described, we hypothesized that malignant mesothelioma might represent an attractive target for endoradiotherapy. However, based on our results, CXCR4 does not seem a promising therapeutic option for patients with progressive, irresectable or chemo-refractory disease.
Limitations of the study include that –also due to the low incidence of mesothelioma- only a limited/small number of patients could be included in the study. Therefore, all conclusions have to be drawn with caution, also given the fact that almost all patients and 4/9 samples included in our study represented the epitheloid subtype. Thus, potentially differential CXCR4 expression by different histologic mesothelioma subtypes (e.g. sarcomatoid mesothelioma) might have been missed.
Furthermore, biopsies were not always obtained on a short-term period compared to the time point of PET imaging. However, the maximum interval between imaging and biopsy was 4 weeks with no treatment administered in between. Thus, we are convinced that therapy-induced changes in receptor expression can be ignored.
To conclude, our data suggest a lower frequency of CXCR4-positivity than previously reported. Prior to targeting this chemokine receptor for therapy, robust cell surface expression should be confirmed by immunohistochemistry of the tumor sample, or whole-body [68Ga]Pentixafor-PET/CT.
MATERIALS AND METHODS
Subjects and research design
Six patients (5 males, 1 female, age 54–80 y; mean, 69 ± 10 y) with histologically proven primary diagnosis of pleural mesothelioma were enrolled.
At the time point of imaging, all patients were treatment-naïve. PET scans were performed for staging purposes ([18F]FDG) and to measure the expression of CXCR4 ([68Ga]Pentixafor) as a potential therapeutic target for a beta-emitter linked analog. After imaging, surgery was performed in all patients. In five subjects, external beam radiation was performed after the surgical procedure. Two patients also received (platinum-based) chemotherapy. Checkpoint inhibitors were administered in one patient. Detailed patient characteristics are given in Supplementary Table 1.
[68Ga]Pentixafor was administered in compliance with The German Medicinal Products Act, AMG §13 2b, and in accordance with the responsible regulatory body (Regierung von Oberfranken). The data analysis was disclosed to the ethics committee of the Universitätsklinikum Würzburg and the need of a formal review was waived. All patients signed written informed consent prior to imaging.
Surgical mesothelioma samples
In addition to the samples available from the patients undergoing imaging, 9 surgical mesothelioma samples were available for histological analysis.
Preparation of [18F]FDG and the chemokine receptor CXCR4 targeting probe [68Ga]Pentixafor
[18F]FDG was synthesized in house with a 16 MeV Cyclotron (GE PETtrace 6; GE Healthcare, Milwaukee, USA) using GE FASTlab methodology according to the manufacturer’s instructions.
Synthesis of [68Ga]Pentixafor was performed in a fully automated, GMP-compliant procedure using a GRP® module (SCINTOMICS GmbH, Fürstenfeldbruck, Germany) connected to a 68Ge/68Ga-generator (Eckert und Ziegler, Berlin, Germany) and equipped with a disposable single-use cassette kit (ABX, Radeberg, Germany), using the standardized labelling sequence previously described [19] and 20 μg of unlabelled Pentixafor (SCINTOMICS GmbH). Before use, the radiopharmaceutical was analyzed according to the monographs 2462 (Gallium Chloride) and 2482 (Gallium Edotreotide) of the European Pharmacopoeia. The radiochemical purity was the tracer was > 98% with a specific activity greater than 5 MBq/μg.
PET imaging
All [68Ga]Pentixafor and [18F]FDG-PET/CT scans were performed on a dedicated PET/CT scanner (Siemens Biograph mCT 64; Siemens Medical Solutions, Erlangen, Germany) after a 4 hour fasting period. For [68Ga]Pentixafor PET, injected activity ranged from 78 to 142 MBq (mean, 123±26 MBq). For standard [18F]FDG-PET which was available in 4/6 patients, 287 ± 22 MBq were administered.
Low dose CT scans for attenuation correction were acquired (35 mAs, 120 keV, a 512 × 512 matrix, 5 mm slice thickness with a total of 201 slices, increment of 30 mm/s, rotation time of 0.5 s, and pitch index of 0.8). The imaging field ranged from the base of the skull to the proximal thighs.
Whole-body scans encompassing 6–7 bed positions were performed 1h after administration of the radiopharmaceutical. All PET images were reconstructed using corrections for attenuation, dead-time, random events and scatter. The PET scanner is periodically checked for calibration accuracy as part of quality control according to published guidelines [20].
Image analysis
Images were visually analyzed by two experienced nuclear medicine specialists (C.L., K.H.). Tumor regions of interest (ROIs) were defined by drawing a standardized 10-mm circular region over the area with the peak tumor activity. Maximum (SUVmax) and mean standardized uptake values (SUVmean) were derived. A reference region was defined by drawing a ROI (diameter of 25 mm) in the cavity of the right ventricle of the heart. The radiotracer concentration in the ROIs was normalized to the injected dose per kilogram body weight of patient to derive the SUVs.
CXCR4 immunohistochemistry (IHC)
Immunohistochemical analysis of CXCR4 expression was performed on paraffin sections (1 μm) derived from biopsies of the primary tumor using an anti-CXCR4 rabbit polyclonal antibody (ab2074; Abcam, Cambridge, UK) and the DAKO en vision system. For evaluation, the immune reactive score – based on the percentage of CXCR4-positive cells multiplied with the staining intensity- was calculated[12]. CXCR4 positivity of vascular epithelium served as internal and adrenocortical tissue as external positive control, respectively [21–23]. Biopsies were obtained within 4 weeks before/after [68Ga]Pentixafor-PET/CT examinations (mean, 20 ± 7 days). In the interval between biopsy/surgery and imaging, no treatment for mesothelioma was administered.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. [68Ga]Pentixafor was administered in compliance with The German Medicinal Products Act, AMG §13 2b, and in accordance with the responsible regulatory body (Regierung von Oberfranken). The data analysis was disclosed to the ethics committee of the Universitätsklinikum Würzburg and the need of a formal review was waived.
Informed consent
Informed consent was obtained from all individual participants included in the study.
ACKNOWLEDGMENTS
We thank Simone Seifert, Michael Schulze-Glück (members of the nuclear medicine PET team) and Christa Albert for their support and assistance.
CONFLICTS OF INTEREST
HJW is founder and shareholder of Scintomics. SKr is CEO of Scintomics. All other authors declare no conflict of interest.
FUNDING
This paper was supported by the University of Wuerzburg as part of the funding program Open Access Publishing.
REFERENCES
1. Bueno R. Mesothelioma clinical presentation. Chest. 1999; 116:444S–445S.
2. Teta MJ, Mink PJ, Lau E, Sceurman BK, Foster ED. US mesothelioma patterns 1973-2002: indicators of change and insights into background rates. Eur J Cancer Prev. 2008; 17:525–534.
3. Marinaccio A, Binazzi A, Bonafede M, Corfiati M, Di Marzio D, Scarselli A, Verardo M, Mirabelli D, Gennaro V, Mensi C, Schallemberg G, Merler E, Negro C, et al, and ReNaM Working Group. Malignant mesothelioma due to non-occupational asbestos exposure from the Italian national surveillance system (ReNaM): epidemiology and public health issues. Occup Environ Med. 2015; 72:648–655.
4. Domanska UM, Kruizinga RC, Nagengast WB, Timmer-Bosscha H, Huls G, de Vries EG, Walenkamp AM. A review on CXCR4/CXCL12 axis in oncology: no place to hide. Eur J Cancer. 2013; 49:219–230.
5. Li T, Li H, Wang Y, Harvard C, Tan JL, Au A, Xu Z, Jablons DM, You L. The expression of CXCR4, CXCL12 and CXCR7 in malignant pleural mesothelioma. J Pathol. 2011; 223:519–530.
6. Demmer O, Gourni E, Schumacher U, Kessler H, Wester HJ. PET imaging of CXCR4 receptors in cancer by a new optimized ligand. ChemMedChem. 2011; 6:1789–1791.
7. Gourni E, Demmer O, Schottelius M, D’Alessandria C, Schulz S, Dijkgraaf I, Schumacher U, Schwaiger M, Kessler H, Wester HJ. PET of CXCR4 expression by a (68)Ga-labeled highly specific targeted contrast agent. J Nucl Med. 2011; 52:1803–1810.
8. Herrmann K, Lapa C, Wester HJ, Schottelius M, Schiepers C, Eberlein U, Bluemel C, Keller U, Knop S, Kropf S, Schirbel A, Buck AK, Lassmann M. Biodistribution and radiation dosimetry for the chemokine receptor CXCR4-targeting probe 68Ga-pentixafor. J Nucl Med. 2015; 56:410–416.
9. Wester HJ, Keller U, Schottelius M, Beer A, Philipp-Abbrederis K, Hoffmann F, Simecek J, Gerngross C, Lassmann M, Herrmann K, Pellegata N, Rudelius M, Kessler H, Schwaiger M. Disclosing the CXCR4 expression in lymphoproliferative diseases by targeted molecular imaging. Theranostics. 2015; 5:618–630.
10. Philipp-Abbrederis K, Herrmann K, Knop S, Schottelius M, Eiber M, Luckerath K, Pietschmann E, Habringer S, Gerngroβ C, Franke K, Rudelius M, Schirbel A, Lapa C, et al. In vivo molecular imaging of chemokine receptor CXCR4 expression in patients with advanced multiple myeloma. EMBO Mol Med. 2015; 7:477–487.
11. Lapa C, Schreder M, Schirbel A, Samnick S, Kortum KM, Herrmann K, Kropf S, Einsele H, Buck AK, Wester HJ, Knop S, Luckerath K. [68Ga]Pentixafor-PET/CT for imaging of chemokine receptor CXCR4 expression in multiple myeloma - Comparison to [18F]FDG and laboratory values. Theranostics. 2017; 7:205–212.
12. Lapa C, Luckerath K, Kleinlein I, Monoranu CM, Linsenmann T, Kessler AF, Rudelius M, Kropf S, Buck AK, Ernestus RI, Wester HJ, Lohr M, Herrmann K. (68)Ga-Pentixafor-PET/CT for Imaging of Chemokine Receptor 4 Expression in Glioblastoma. Theranostics. 2016; 6:428–434.
13. Lapa C, Luckerath K, Rudelius M, Schmid JS, Schoene A, Schirbel A, Samnick S, Pelzer T, Buck AK, Kropf S, Wester HJ, Herrmann K. [68Ga]Pentixafor-PET/CT for imaging of chemokine receptor 4 expression in small cell lung cancer - initial experience. Oncotarget. 2016; 7:9288–9295. https://doi.org/10.18632/oncotarget.7063.
14. Lapa C, Reiter T, Werner RA, Ertl G, Wester HJ, Buck AK, Bauer WR, Herrmann K. [(68)Ga]Pentixafor-PET/CT for Imaging of Chemokine Receptor 4 Expression After Myocardial Infarction. JACC Cardiovasc Imaging. 2015; 8:1466–1468.
15. Schmid JS, Schirbel A, Buck AK, Kropf S, Wester HJ, Lapa C. [68Ga]Pentixafor-Positron Emission Tomography/Computed Tomography Detects Chemokine Receptor CXCR4 Expression After Ischemic Stroke. Circ Cardiovasc Imaging. 2016; 9:e005217.
16. Vag T, Gerngross C, Herhaus P, Eiber M, Philipp-Abbrederis K, Graner FP, Ettl J, Keller U, Wester HJ, Schwaiger M. First Experience with Chemokine Receptor CXCR4-Targeted PET Imaging of Patients with Solid Cancers. J Nucl Med. 2016; 57:741–746.
17. Davidson B, Dong HP, Holth A, Berner A, Risberg B. Chemokine receptors are infrequently expressed in malignant and benign mesothelial cells. Am J Clin Pathol. 2007; 127:752–759.
18. Herrmann K, Schottelius M, Lapa C, Osl T, Poschenrieder A, Hanscheid H, Luckerath K, Schreder M, Bluemel C, Knott M, Keller U, Schirbel A, Samnick S, et al. First-in-Human Experience of CXCR4-Directed Endoradiotherapy with 177Lu- and 90Y-Labeled Pentixather in Advanced-Stage Multiple Myeloma with Extensive Intra- and Extramedullary Disease. J Nucl Med. 2016; 57:248–251.
19. Martin R, Juttler S, Muller M, Wester HJ. Cationic eluate pretreatment for automated synthesis of [68Ga]CPCR4.2. Nucl Med Biol. 2014; 41:84–89.
20. Boellaard R, Hristova I, Ettinger S, Stroobants S, Chiti A, Bauer A, Tatsch K, Bourguet P, Bean J, Oyen W. Initial experience with the EANM accreditation procedure of FDG PET/CT devices. Eur J Cancer. 2011; 47:S8.
21. Gupta SK, Lysko PG, Pillarisetti K, Ohlstein E, Stadel JM. Chemokine receptors in human endothelial cells. Functional expression of CXCR4 and its transcriptional regulation by inflammatory cytokines. J Biol Chem. 1998; 273:4282–4287.
22. Molino M, Woolkalis MJ, Prevost N, Pratico D, Barnathan ES, Taraboletti G, Haggarty BS, Hesselgesser J, Horuk R, Hoxie JA, Brass LF. CXCR4 on human endothelial cells can serve as both a mediator of biological responses and as a receptor for HIV-2. Biochim Biophys Acta. 2000; 1500:227–240.
23. Fischer T, Nagel F, Jacobs S, Stumm R, Schulz S. Reassessment of CXCR4 chemokine receptor expression in human normal and neoplastic tissues using the novel rabbit monoclonal antibody UMB-2. PLoS One. 2008; 3:e4069.