
INTRODUCTION
Pancreatic cancer (PC) is the fourth leading cause of cancer-related death in the United States [1]. Owing to late stage at the time of diagnosis, there are just 10%-20% of patients eligible for surgical treatment [2]. Although the surgical procedure of pancreatic cancer over the last decades has improved strongly, it needs some more effective treatments and adjuvant therapies against PC.
The relationship between PC and diabetes mellitus (DM) has been increasingly recognized over the past decades. Studies suggest that DM plays a pivotal role in cancer risk and progression [3–5]. Although we have not fully understood the mechanisms of increased risk of cancer incidence with DM, hyperinsulinemia may influence the neoplastic process through its effects on enhancing cancer cell proliferation, survival, and invasion and inhibiting apoptosis in the insulin-like growth factor-I (IGF-I) signaling pathway [6, 7]. There are an increasing number of experimental evidence and epidemiologic studies to show that ADMs may modify the prognosis of PC. Some studies suggest that metformin may improve outcome of patients with diabetes and pancreatic cancer [8–13], whereas others have not revealed beneficial effect [14–18]. Besides, some studies suggest that insulin may highlight risk of PC mortality [19, 20], whereas others have not affected the survival [8, 11]. Due to controversial results among studies, we thus carry out this meta-analysis to investigate the prognostic value of ADMs use (as compared with non-user) among PC patients.
RESULTS
Description of the included studies
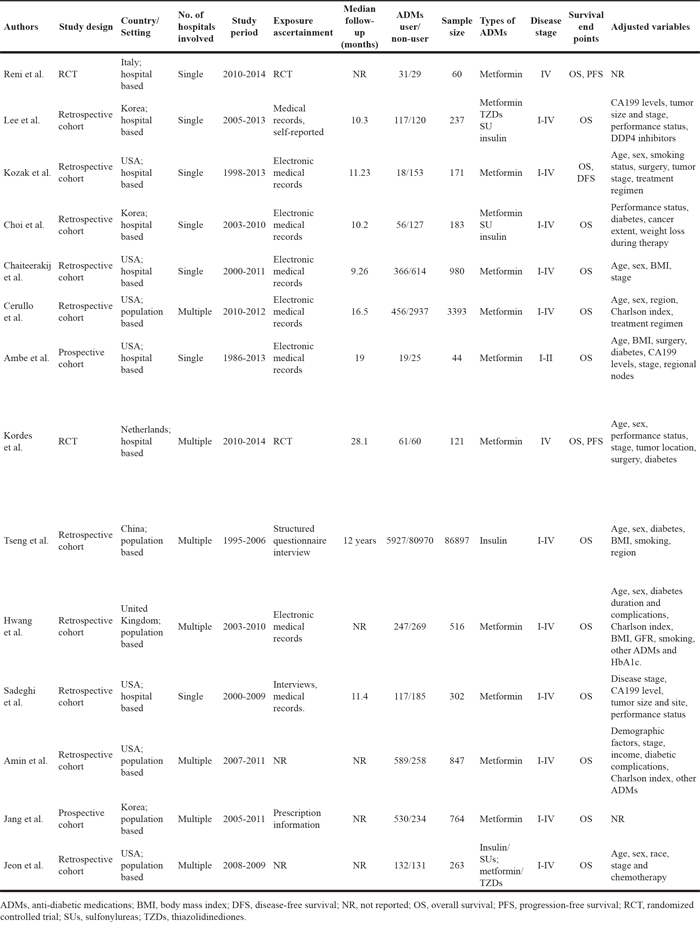
The initial database search yielded a total of 3326 references for eligibility. After excluding the duplicates and screening the remaining title and abstract, 42 potentially relevant studies were identified for further review. After selection, a total of 14 publications met our inclusion criteria (Figure 1). The clinical features of included studies were summarized in Table 1. In summary, 13 studies investigated the survival outcomes for patients of metformin use, 5 for insulin use, 2 for SUs use and 2 for TZDs use. The median follow-up time ranged from 0.77 to 12 years. 5 studies were carried out in USA, 3 in Europe and 2 in Asia. Several cohorts were adjusted for some conventional influential factors, including age, sex, disease stage. Six studies involved PC patients with I-IV disease stages, and two with stage IV. Assessment of methodological quality for cohort studies yielded a score range of 7 to 9, and 7 of 12 studies had a score of 8 or above (Supplementary Table 1).
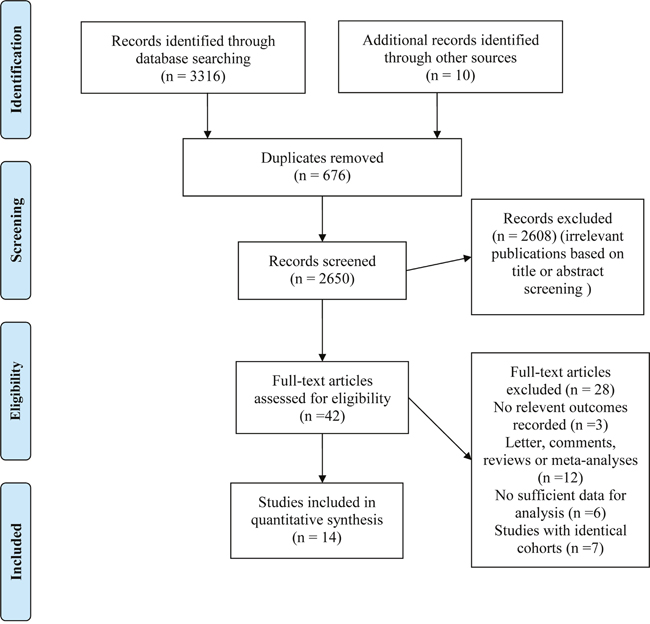
Figure 1: Flow diagram of the selection process of studies investigating effect of anti-diabetic medications use on pancreatic cancer survival.
Table 1: Baseline characteristics of the included studies on survival outcomes of anti-diabetic medications use for pancreatic cancer patients
Metformin use and PC survival
The combined HR for the OS comparing metformin use versus non-use was 0.77 (95% CI=0.68-0.87) with moderate inter-study heterogeneity (I2=52.9%, p=0.02) (Figure 2A) for cohort studies. Figure 2B presents the HR (HR=1.22; 95% CI=0.76-1.95) for PFS. No significant survival benefit was noted for randomized controlled trials (RCTs) (HR=1.20, 95% CI=0.84-1.72).
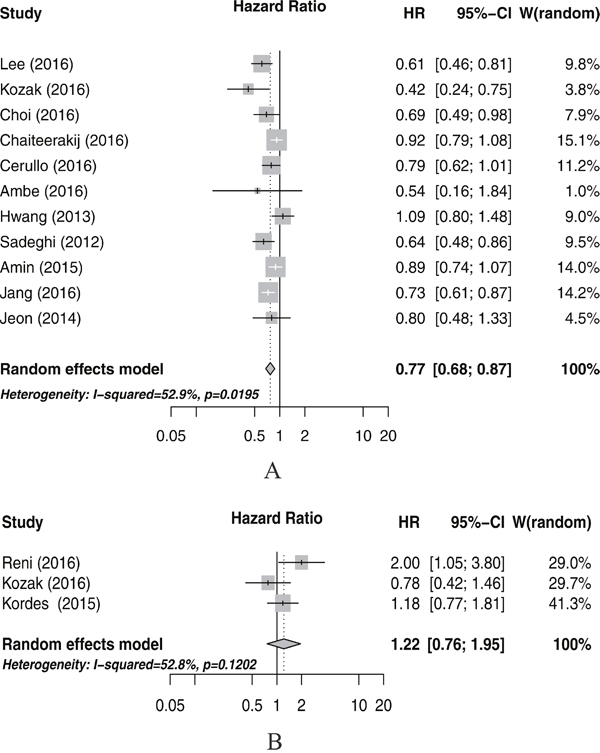
Figure 2: Meta-analysis of the associations between metformin use and pancreatic cancer overall survival (A), and progression-free surival (B). CI, confidence interval; HR, hazard ratio; W (random): Weights (random effects model).
We summarized the subgroup analyses for OS in Table 2 to further test potential sources of heterogeneity among certain major clinical characteristics of the included studies. The pooled HRs for the majority of the subgroups did not change significantly stratified by some major study characteristics, including the study design and setting, study country, the number of hospitals, sample size, adjusted variables or the scores of Newcastle–Ottawa Quality Assessment Scale. A possible interaction was found in the subgroup of sample size. Results of analyses limited to studies with some of the main variable adjusted (age, sex and tumor stage) are also presented in Table 2. For studies with these three variables adjusted, a null prognostic association of metformin use was noted. Nevertheless, further studies should be conducted to examine the true survival benefit of metformin in PC patients due to the small number of studies involved in these subgroups.
Table 2: Subgroup analyses of the associations between metformin use and overall survival for cohort studies
Comparison variables |
Overall survival |
|||
|---|---|---|---|---|
No. of studies |
I2 statistics; % |
HR (95% CI) |
Pinteration |
|
Total |
11 |
52.9 |
0.77(0.68 - 0.87) |
NA |
Study design |
0.534 |
|||
Prospective cohort |
2 |
0 |
0.72(0.61 - 0.86) |
|
Retrospective cohort |
9 |
58.9 |
0.78(0.67 -0.90) |
|
Study setting |
0.111 |
|||
Hospital based |
6 |
64.5 |
0.67(0.53 - 0.85) |
|
Population based |
5 |
33.6 |
0.84(0.73 - 0.96) |
|
Study region |
0.214 |
|||
USA |
7 |
47.2 |
0.78(0.67 - 0.92) |
|
Europe |
1 |
1.09(0.80 - 1.48) |
||
Asia |
3 |
0 |
0.69(0.60 - 0.79) |
|
Hospital number |
0.111 |
|||
Single |
6 |
64.5 |
0.67(0.53 - 0.85) |
|
Multiple |
5 |
33.6 |
0.84(0.73 -0.96) |
|
Sample size |
0.0024 |
|||
≥500 |
5 |
44.1 |
0.86(0.76 -0.97) |
|
<500 |
6 |
0 |
0.63(0.54 - 0.74) |
|
Main variable adjusted* |
0.276 |
|||
Yes |
5 |
57.8 |
0.83(0.68 -1.03) |
|
No |
6 |
30.8 |
0.73(0.64 -0.83) |
|
NOS scale |
0.359 |
|||
≥8 |
6 |
59.4 |
0.73(0.59 - 0.90) |
|
<8 |
5 |
36.2 |
0.82(0.71 - 0.94) |
|
CI, confidence interval; HR, hazard ratio; Main variable adjusted*, Age, sex, stage; NA; not available.
Sensitivity analysis by omitting one single study each time and pooling the others indicated that the pooled HRs was not significantly altered. Funnel plot for publication bias did not show asymmetry (Figure 3). Further Egger’s test (P=0.135) or Begg’s test (P=0.436) also did not found a certain degree publication bias.
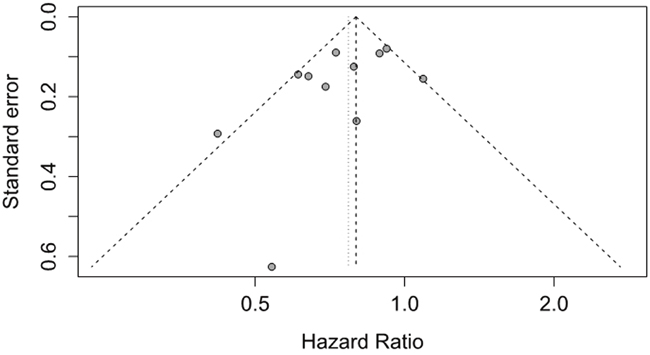
Figure 3: Funnel plot of studies investigating association between metformin use and pancreatic cancer survival for cohort studies.
Other ADMs use and PC survival
Five studies investigated the impact of insulin use and PC survival and there was no significant association between insulin use and PC survival (HR=1.18, 95% CI=0.83-1.69; Figure 4A). We also did not find significant association between SUs (HR=1.03, 95% CI=0.81-1.30; Figure 4B) or TZDs (HR=0.84, 95% CI=0.58-1.22; Figure 4C) use and PC survival.
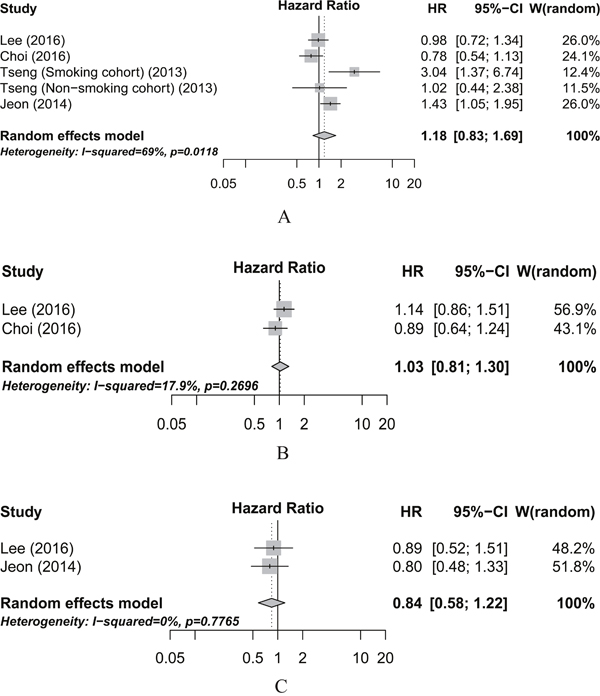
Figure 4: Meta-analysis of the associations between insulin (A), sulfonylureas (B), and thiazolidinediones (C) use and pancreatic cancer overall survival. CI, confidence interval; HR, hazard ratio; W (random): Weights (random effects model).
DISCUSSION
This meta-analysis investigated the association between ADMs (metformin, insulin, SUs and TZDs) treatment and survival of PC. We found metformin treatment was significantly associated with favorable OS of PC patients (HR=0.77, 95% CI=0.68-0.87) in cohort studies, but was not significantly associated with PFS (HR=1.22; 95% CI=0.76-1.95) for RCTs. We also found no survival benefits of other ADMs, such as insulin, SUs or TZDs, for PC patients.
Several potential mechanisms may explain the associations for the fact that conventional ADMs may alter the risk of multiple malignancies. It was reported that metformin has been shown to play an important anticancer role in multiple ways including insulin-dependent or independent manners [21]. A recent study found that SUs can induce cell proliferation and had an effect of carcinogenesis by promoting insulin secretion [22]. Moreover, previous in vitro studies showed that TZDs had an impact on cell growth arrest and apoptosis and the inhibition of cancer cell invasion [23].
Several important strengths of this meta-analysis should be addressed. Firstly, to the best of our knowledge, this is the first systematic review regarding the associations between the use of ADMs and prognosis of PC. Secondly, comprehensive and reproducible search strategies were developed to identify all relevant studies or trials in the major databases without language limitations. Thirdly, we investigated the most commonly used ADMs including metformin, SUs, TZDs and insulin and conducted a meta-analysis for both RCTs and cohort studies. Fourthly, more than 90000 participants were included to quantitatively assess the association between ADMs use and PC prognosis, which was the most comprehensive synthesis of the evidence on this topic ever today. Finally, several subgroup analyses were carried out for some of the important variables, such as study design and setting, research region, number of research hospital, main variable adjusted and quality score. The results showed consistency across subgroups.
Still there are limitations in our systematic review. Firstly, the number of studies for each medication involved in this meta-analysis was relatively small except for metformin, and thus it is difficult to draw definite conclusions for the limited statistical power in SUs, TZDs or insulin subset. Secondly, almost none of the included studies had dose or duration-response analysis for certain ADMs, so it is impossible for us to perform this kind of analysis. Therefore, further study should be focused on this aspect. Thirdly, although some major confounders including age, sex and disease stage were identified and adjusted for some of the included studies, some other variables (such as tumor size, body mass index or chemotherapy) could influence our exploration of associations between ADMs and PC survival. Last but not the least, although we did not find significant publication bias for metformin subset in cohort studies, we could not totally exclude potential impact of unpublished studies on the pooled results, which might have resulted in reporting bias. However, the adjusted estimates of the results using the trim and fill methods remained unchanged, indicating the stability of our analysis.
In summary, the results from this meta-analysis revealed that in cohort studies, metformin, not other ADMs was associated with improved OS in PC patients. However, due to limited number of studies investigating other ADMs, further large-scale studies are warranted to determine these associations.
MATERIALS AND METHODS
Literature search and study selection
Based on the PRISMA statement [24], we performed a comprehensive literature search in Pubmed and Embase databases up to August 2016 for relevant citations without language restrictions. We used the search strategies (Supplementary Table 2 and Table 3) that included Medical Subject Headings and Emtree headings combined key words relating to the prognostic effect of ADMs among PC patients. We also manually scanned the reference lists from the extracted relevant research papers, previous reviews and meta-analysis for additional possible publications.
We included published studies providing aggregate data if they met the following criteria: (1) evaluated any prognostic information in PC patients comparing ADMs users with non-users, (2) reported a summary statistic of hazard ratios (HRs) with 95% confidence intervals (CIs) or provided date for calculation as described by Parmar et al [25]. RCTs or observational studies were eligible for this meta-analysis. If there were more than one studies from the same cohort, we selected the most detailed or recent one for analysis. All the studies reporting prognostic information, including overall survival (OS), and progression-free survival (PFS), were selected in the main analyses (Supplementary Table 4). Two independent investigators (Zhou and Gong) conducted the study selection from eligible studies.
Data extraction
Two independent investigators (Zhou and Gong) selected articles and extracted data from eligible studies, evaluated the quality of each study and any discrepancies were resolved by a consensus discussion with a third investigator (Tan). The characteristics recorded were the first author’s last name, publication year, country of the population studied, study design, study setting, number of hospitals involved, time period of study, information source for exposure ascertainment and outcome assessment, total number of persons in each group (exposed vs. not exposed), sample size, types of ADMs, stage, mean F/U (months), survival endpoints and adjustment variables HR, and 95% confidence intervals (CIs) with adjustment for confounding factors. The methodological quality of each study was evaluated using the Newcastle-Ottawa quality assessment scale [26], in which three domains including cohort selection, comparability, and outcome were evaluated with a score range of 0 to 9 with nine representing the highest quality.
Statistical analysis
We used STATA statistical software (version 12.0, StataCorp LP, College Station, TX) and R statistical software (version 3.3.1) to perform the meta-analysis. Survival estimates with full adjustments for known confounders of included studies were abstracted. Summary data reporting HRs with corresponding 95% CIs estimated from Cox proportional hazards models were pooled with random-effects model [27]. The data regarding the association of ADMs (use vs. no use) with survival outcomes were pooled separately. We used the Cochrane Q statistic (with a P value less than 0.10 considering statistically significant) and the I2 statistic (with an I2 exceeding 50% indicating significant heterogeneity) to test for between-study heterogeneity [28]. Metformin usage and OS for PC patients were explored for primary meta-analysis. Other outcome measures such as PFS and Disease-free survival (DFS) were also evaluated. Owing to the limited studies for PFS and DFS, we combined the data of PFS and DFS as one outcome for the meta-analysis. We performed sensitivity analyses to explore the reasons for statistical heterogeneity. The risk of publication bias was assessed visually by inspecting of a funnel plot and statistically by using Egger's or Begg's regression model [29]. We further ascertained the number of missing studies using Duval and Tweedie’s trim and fill method to adjust the summary hazard ratio based on all the studies including the hypothesized missing ones [30]. All statistical analyses were two-sided and a P-value less than 0.05 was considered significant.
Abbreviations
ADMs: anti-diabetic medications; SUs: sulfonylureas; TZDs: thiazolidinediones; DM: diabetes mellitus; PC: Pancreatic cancer; HRs: hazard ratios; CIs: confidence intervals; OS: overall survival; PFS: progression-free survival. RCTs: randomized controlled trials.
CONFLICTS OF INTEREST
The authors declare no competing financial interests.
REFERENCES
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016; 66:7–30.
2. Ryan DP, Hong TS, Bardeesy N. Pancreatic adenocarcinoma. N Engl J Med. 2014; 371:1039–49.
3. Chiu CC, Huang CC, Chen YC, Chen TJ, Liang Y, Lin SJ, Chen JW, Leu HB, Chan WL. Increased risk of gastrointestinal malignancy in patients with diabetes mellitus and correlations with anti-diabetes drugs: a nationwide population-based study in Taiwan. Intern Med. 2013; 52:939–46.
4. Ben Q, Xu M, Ning X, Liu J, Hong S, Huang W, Zhang H, Li Z. Diabetes mellitus and risk of pancreatic cancer: A meta-analysis of cohort studies. Eur J Cancer. 2011; 47:1928–37.
5. Huxley R, Ansary-Moghaddam A, Berrington de González A, Barzi F, Woodward M. Type-II diabetes and pancreatic cancer: a meta-analysis of 36 studies. Br J Cancer. 2005; 92:2076–83.
6. Kuuselo R, Savinainen K, Azorsa DO, Basu GD, Karhu R, Tuzmen S, Mousses S, Kallioniemi A. Intersex-like (IXL) is a cell survival regulator in pancreatic cancer with 19q13 amplification. Cancer Res. 2007; 67:1943–49.
7. Asano T, Yao Y, Shin S, McCubrey J, Abbruzzese JL, Reddy SA. Insulin receptor substrate is a mediator of phosphoinositide 3-kinase activation in quiescent pancreatic cancer cells. Cancer Res. 2005; 65:9164–68.
8. Lee SH, Yoon SH, Lee HS, Chung MJ, Park JY, Park SW, Song SY, Chung JB, Bang S. Can metformin change the prognosis of pancreatic cancer? Retrospective study for pancreatic cancer patients with pre-existing diabetes mellitus type 2. Dig Liver Dis. 2016; 48:435–40.
9. Kozak MM, Anderson EM, von Eyben R, Pai JS, Poultsides GA, Visser BC, Norton JA, Koong AC, Chang DT. Statin and Metformin Use Prolongs Survival in Patients With Resectable Pancreatic Cancer. Pancreas. 2016; 45:64–70.
10. Jang WI, Kim MS, Kang SH, Jo AJ, Kim YJ, Tchoe HJ, Park CM, Kim HJ, Choi JA, Choi HJ, Paik EK, Seo YS, Yoo HJ, et al. Association between metformin use and mortality in patients with type 2 diabetes mellitus and localized resectable pancreatic cancer: a nationwide population-based study in korea. Oncotarget. 2017; 8:9587–96. https://doi.org/10.18632/oncotarget.14525.
11. Choi Y, Kim TY, Oh DY, Lee KH, Han SW, Im SA, Kim TY, Bang YJ. The Impact of Diabetes Mellitus and Metformin Treatment on Survival of Patients with Advanced Pancreatic Cancer Undergoing Chemotherapy. Cancer Res Treat. 2016; 48:171–79.
12. Cerullo M, Gani F, Chen SY, Canner J, Pawlik TM. Metformin Use Is Associated with Improved Survival in Patients Undergoing Resection for Pancreatic Cancer. J Gastrointest Surg. 2016; 20:1572–80.
13. Sadeghi N, Abbruzzese JL, Yeung SC, Hassan M, Li D. Metformin use is associated with better survival of diabetic patients with pancreatic cancer. Clin Cancer Res. 2012; 18:2905–12.
14. Reni M, Dugnani E, Cereda S, Belli C, Balzano G, Nicoletti R, Liberati D, Pasquale V, Scavini M, Maggiora P, Sordi V, Lampasona V, Ceraulo D, et al. (Ir)relevance of Metformin Treatment in Patients with Metastatic Pancreatic Cancer: An Open-Label, Randomized Phase II Trial. Clin Cancer Res. 2016; 22:1076–85.
15. Chaiteerakij R, Petersen GM, Bamlet WR, Chaffee KG, Zhen DB, Burch PA, Leof ER, Roberts LR, Oberg AL. Metformin Use and Survival of Patients With Pancreatic Cancer: A Cautionary Lesson. J Clin Oncol. 2016; 34:1898–904.
16. Kordes S, Pollak MN, Zwinderman AH, Mathôt RA, Weterman MJ, Beeker A, Punt CJ, Richel DJ, Wilmink JW. Metformin in patients with advanced pancreatic cancer: a double-blind, randomised, placebo-controlled phase 2 trial. Lancet Oncol. 2015; 16:839–47.
17. Amin S, Mhango G, Lin J, Boffetta P, Wisnivesky J, Lucas A. Metformin use does not improve survival among diabetics with pancreatic adenocarcinoma: A population-based analysis. Am J Gastroenterol. 2015; 110:S17.
18. Hwang AL, Haynes K, Hwang WT, Yang YX. Metformin and survival in pancreatic cancer: a retrospective cohort study. Pancreas. 2013; 42:1054–59.
19. Jeon CY, Pandol SJ, Goodman MT. Survival time in pancreatic cancer patients with metabolic syndrome varies by use of insulin and statins. Cancer Res. 2014; 74:2173.
20. Tseng CH. Diabetes, insulin use, smoking, and pancreatic cancer mortality in Taiwan. Acta Diabetol. 2013; 50:879–86.
21. Gallagher EJ, LeRoith D. Diabetes, cancer, and metformin: connections of metabolism and cell proliferation. Ann N Y Acad Sci. 2011; 1243:54–68.
22. Bowker SL, Majumdar SR, Veugelers P, Johnson JA. Increased cancer-related mortality for patients with type 2 diabetes who use sulfonylureas or insulin. Diabetes Care. 2006; 29:254–58.
23. Okumura T. Mechanisms by which thiazolidinediones induce anti-cancer effects in cancers in digestive organs. J Gastroenterol. 2010; 45:1097–102.
24. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010; 8:336–41.
25. Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat Med. 1998; 17:2815–34.
26. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010; 25:603–05.
27. van Houwelingen HC, Arends LR, Stijnen T. Advanced methods in meta-analysis: multivariate approach and meta-regression. Stat Med. 2002; 21:589–624.
28. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002; 21:1539–58.
29. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997; 315:629–34.
30. Duval S, Tweedie R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000; 56:455–63.