
INTRODUCTION
Hepatocellular carcinoma (HCC) ranks fifth among the most common cancer globally and is the third most frequent cause of cancer deaths [1–2]. A common complication of HCC is the Portal vein tumor thrombus (PVTT) that results in a poor median survival of 2.7–4.0 months and is reported in 64.7% cases at autopsy [3–6]. The poor prognosis associated with PVTT is due to increased risk of tumor spread; variceal hemorrhage as a result of increased portal venous blood pressure; and complications including ascites, jaundice, hepatic encephalopathy, and liver failure due to decreased portal flow [7, 8]. Further, since PVTT is a contraindicator for transplantation and curative resection according to the HCC treatment guidelines, the treatment options are limited [9–10]. Therefore, the standard management for HCC patients with PVTT is controversial [8, 10, 11].
The efficacy of sorafenib, which is the recommended therapy for HCC patients with PVTT according to the Barcelona Clinic Liver Cancer staging system, is limited [12–13]. However, patients with PVTT that underwent transarterial chemoembolization (TACE) in addition to sorafenib demonstrated better survival according to some studies [14–15]. Therefore, TACE therapy is considered for advanced-stage HCC patients [1, 16–17]. However, since sorafenib is expensive, the majority of patients in China with advanced HCC (with PVTT) cannot afford such treatment, and therefore, there is an urgent need for an alternative and more cost-effective treatment.
Yang et al. reported that TACE in combination with endovascular implantation of a 125iodine seed strand was a feasible and effective treatment for HCC patients with PVTT [19]. Some studies reported computed tomography (CT)-guided 125iodine implantation in HCC patients with PVTT [20–21]. The two methods are different, and direct CT-guided 125iodine implantation in PVTT is technically easier to perform. However, these studies included very few cases of CT-guided 125iodine seed implantation in PVTT without any control group or analysis of long-term outcomes.
Thus, we evaluated the safety and efficacy of TACE combined with direct CT-guided 125iodine implantation in PVTT (TACE-125iodine) in a retrospective cohort study of HCC patients that had PVTT only in the right or left portal vein branch and absent in the main portal vein.
RESULTS
Patient characteristics
Out of 137 patients with unresectable HCC with type B PVTT that underwent either TACE-125iodine or TACE only, 37 were excluded because they did not meet the inclusion criteria (Figure 1). As a result, we studied 100 patients (TACE-125iodine, n=50; TACE only, n=50) that qualified for our analysis. Detailed baseline patient characteristics are shown in Table 1. The baseline characteristics between the TACE-125iodine and the TACE only groups were not statistically different. The mean follow-up duration for the TACE-125iodine group was 24.2 months (range, ≤1 month to 56 months) and 6.3 months (range, ≤1 month to 18 months) for the TACE only group. During the follow-up, 44 of the 50 patients (88%) in the TACE-125iodine group and 49 of the 50 patients (98%) in the TACE only group died. Five (10%) of the 50 patients underwent repeated 125iodine seed implantation with a mean average of 1.3 (range, 1–2) procedures per patient in the TACE-125iodine group. Thirty-six of the 50 patients (78%) in the TACE-125iodine group and 33 of the 50 patients (73%) in the TACE only group underwent repeated TACE, with a mean average of 3.6 (range, 1–8) and 3.1 (range, 1–6), respectively (Table 2). The bilirubin level increased at 4 weeks after 125iodine seed implantation but recovered to baseline values at 8 weeks (Table 3 and Table 4).
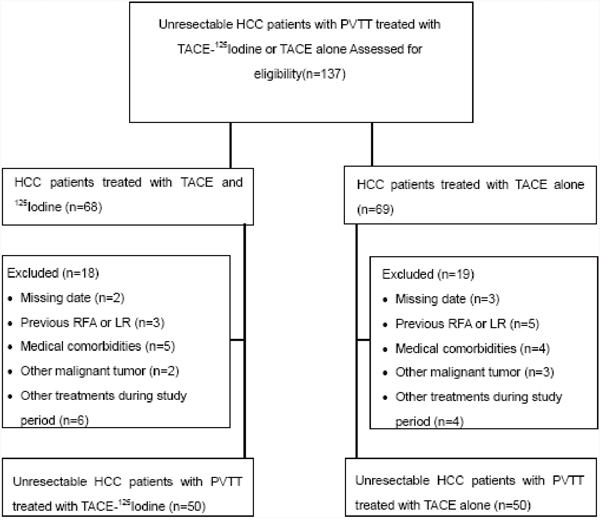
Figure 1: Flow diagram shows exclusion citeria.
Table 1: Baseline Patient Characteristics
Characteristic |
TACE |
TACE-125I |
P Value |
|---|---|---|---|
Sex |
.603* |
||
Male |
40(80) |
42(84) |
|
Female |
10(20) |
8(16) |
|
Age(y)† |
45.4±5.2 |
47.6±6.3 |
.321‡ |
ECOG performance |
.689* |
||
0 |
25(50) |
27(54) |
|
1-2 |
25(50) |
23(46) |
|
Cause of liver disease |
.455* |
||
Hepatitis B |
40(80) |
42(84) |
|
Hepatitis C |
8(16) |
7(14) |
|
Other |
2(4) |
1(2) |
|
Child-Pugh score |
.564* |
||
A |
44(88) |
42(84) |
|
B |
6(12) |
8(16) |
|
Morphology |
.641* |
||
Massive |
27(54) |
26(52) |
|
Multi-nodular |
23(46) |
24(48) |
|
Maximum diameter |
.638‡ |
||
>5cm |
31(62) |
30(60) |
|
≤5 cm |
19(38) |
20(40) |
|
Baseline laboratory test result† |
|||
Total bilirubin level(μmol/L) |
22.1±3.4 |
21.3±5.2 |
.576‡ |
Albumin level (g/L) |
36.4±2.3 |
35.2±3.1 |
.645‡ |
α-Fetoprotein level (ng/mL) |
.688* |
||
>400 |
28(56) |
26(52) |
|
≤400 |
22(44) |
24(48) |
|
Extrahepatic spread |
.309* |
||
Lymph nodes |
10(20) |
12(25) |
|
Lung |
5(10) |
4(8) |
|
Boes |
2(4) |
2(4) |
|
Suprarenal gland |
1(2) |
1(2) |
Note: Unless indicated, date are numbers of patients, and numbers in parentheses are percentages.
ECOG=Eastern Cooperative Oncology Group.
* Pearson χ2 test was used.
†Date are mean±standard deviation.
‡Independent-samples t test was used.
Table 2: Times of TACE procedures per patient in two groups
Treatment method |
No.of Patients(n=100) |
Times of TACE |
P Value* |
|---|---|---|---|
TACE |
50 |
3.6±0.5 |
0.658 |
TACE-125I |
50 |
3.1±1.1 |
Note: Date in parentheses are 95%CIs. ECOG=Eastern Cooperative Oncology Group.
* Independent-samples t test was used.
Table 3: Liver Function Changes 4 Weeks after Treatment in the TACE-125I Group
Liver Function Test |
Pretreatment |
4 Weeks after Treatment |
P Value* |
|---|---|---|---|
Total bilirubin level(μmol/L) |
21.3±5.2 |
42.5±3.5 |
.023 |
Albumin level (g/L) |
35.2±3.1 |
36.1±2.1 |
.053 |
Prothrombin time (sec) |
12.8±0.5 |
13.2±0.4 |
.062 |
Note: Unless indicated, date are mean±standard deviation.
*Paired-Samples T test was used
Table 4: Liver Function Changes 8 Weeks after Treatment in the TACE-125I Group
Liver Function Test |
Pretreatment |
8 Weeks after Treatment |
P Value* |
|---|---|---|---|
Total bilirubin level(μmol/L) |
21.3±5.2 |
22.0±0.5 |
.623 |
Albumin level (g/L) |
35.2±3.1 |
37.1±1.1 |
.453 |
Prothrombin time(sec) |
12.8±0.5 |
12.8±1.4 |
.762 |
Note: Unless indicated, date are mean±standard deviation.
*Paired-Samples T test was used
Adverse events related to TACE
Minor TACE-related adverse events like new ascites, liver dysfunction, fever, abdominal pain, and nausea or vomiting were reported in most patients of both groups. The adverse events were treated symptomatically in the hospital, and all patients recovered from the events. Severe adverse events such as spontaneous bacterial peritonitis, gastrointestinal hemorrhage, liver abscess, or pulmonary or cerebral oil embolization were not encountered during or after the TACE procedure in any patient.
Adverse events related to 125iodine seed implantation
Few acute adverse events were reported due to 125iodine seed implantation. Three patients had pneumothorax with collapsed lung (<30% of the ipsilateral lung), but recovered after conservative treatment. In four cases, minor subcapsular liver hemorrhage was observed, which was treated conservatively with success. In two cases, seed floatation to the normal liver parenchyma was observed that did not require any medical management. Apart from these, other severe adverse events such as hemorrhage, bile fistula, abscess formation, acute peritonitis, and liver failure, were not observed in relation to125iodine seed implantation.
Intrahepatic lesions and PVTT response
During the last follow-up, two experienced radiologists (HLL and CYG) evaluated the intrahepatic lesions response rate according to the mRECIST assessment of HCC [25]. The intrahepatic lesions control rate was 86% for the TACE-125iodine group and 88% for the TACE alone group. The intrahepatic lesions responses are shown in Table 5. There were no significant differences among the two groups in relation to the objective response rate of intrahepatic lesions (P=0.766).
Table 5: Intrahepatic Lesions Responses for the Two Groups
Intrahepatic lesions responses |
TACE-125I |
TACE-alone |
P Value |
|---|---|---|---|
Total patients |
50 |
50 |
|
Complete response |
0 |
0 |
|
Partial response |
34 |
36 |
|
Stable disease |
9 |
8 |
|
Progressive disease |
7 |
6 |
|
Disease control rate (%) |
86 |
88 |
0.766 |
Note: Disease control rate (DCR) was calculated with the following equation: DCR = (SD + PR + CR)/N, where SD is number of patients with stable disease, PR is number of patients with partial response, and CR is number of patients with complete response. P values<.005 indicated a significant difference (Pearson Chi-Square test).
A new system was used to categorize the PVTT responses based on CT scans or MRI. The categories were as follows: (1) Complete response (CR) = PVTT disappearance and restored portal vein blood flow; (2) Partial response (PR) = PVTT disappearance or a >30% reduction in thrombus in the greatest cross-sectional area and improved portal vein blood flow; (3) Stable disease (SD) = <30% reduction in thrombus in the greatest cross-sectional area; and (4) Progressive disease (PD) = extended thrombus [19]. The PVTT responses are shown in Table 6. The PVTT control rate for the TACE-125iodine group was 78% compared to 18% in the TACE only group (P<0.01).
Table 6: Tumor Responses in PVTT for the Two Groups
Tumor Response in PVTT |
TACE-125I |
TACE-alone |
P Value |
|---|---|---|---|
Total patients |
50 |
50 |
|
Complete response |
0 |
0 |
|
Partial response |
20 |
1 |
|
Stable disease |
19 |
8 |
|
Progressive disease |
11 |
41 |
|
Disease control rate (%) |
78 |
18 |
<.001 |
Note: Disease control rate (DCR) was calculated with the following equation: DCR = (SD + PR + CR)/N, where SD is number of patients with stable disease, PR is number of patients with partial response, and CR is number of patients with complete response. P values<.005 indicated a significant difference (Pearson Chi-Square test).
The median OS in the TACE-125iodine group was 13.1 months (95% confidence interval [CI]: 10.1-15.1) and 6.0 months (95% CI: 4.3-7.7) in the TACE only group (P<0.01; Figure 2). Univariate analyses revealed that patients undergoing TACE-125iodine treatment demonstrated better OS than the TACE only patients (Table 7; P<0.01). On the basis of these findings, multivariate analysis demonstrated that treatment method was an independent prognostic factor for OS (Table 8).
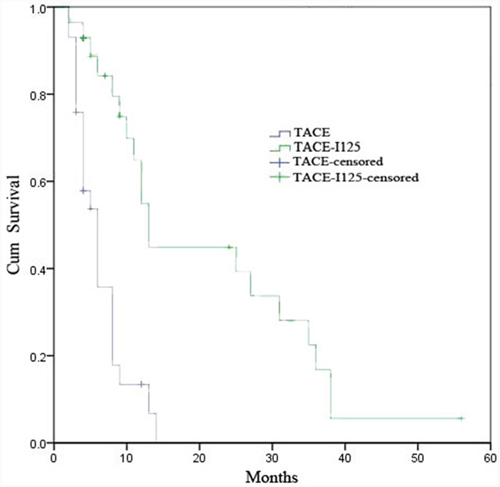
Figure 2: Kaplan-Melier cureves of OS in patients with HCC and PVTT who underwent TACE-125iodine or TACE.
Table 7: Univariate Analysis of Prognostic Factor for OS
Factor |
No.of Patients(n=100) |
Median OS(mo) |
P Value* |
|---|---|---|---|
ECOG performance |
.532 |
||
0 |
46 |
8.2(4.7,12.1) |
|
1-2 |
54 |
8.3(6.8,9.6) |
|
Child-Pugh score |
.653 |
||
A |
75 |
8.3(7.2,9.8) |
|
B |
25 |
8.3(5.6,11.6) |
|
Treatment method |
<.01 |
||
TACE |
50 |
6.0(4.3,7.7) |
|
TACE-125I |
50 |
13.0(10.1,15.1) |
|
α-Fetoprotein level (ng/mL) |
.687 |
||
>400 |
55 |
8.5(7.3,11.3) |
|
≤400 |
45 |
8.6(7.2,11.6) |
Note: Date in parentheses are 95%CIs. ECOG=Eastern Cooperative Oncology Group.
* Log-rank test was used
Table 8: Multivariate Analysis of Prognostic Factor for OS
Factor |
Hazard Ratio# |
P Value* |
|---|---|---|
Treatment method |
<.001 |
|
TACE |
2.54(1.52,3.75) |
|
TACE-125I |
1 |
Note: Date in parentheses are 95%CIs.
* Cox regression was used
DISCUSSION
Song et al. reported that median OS in HCC patients with PVTT treated with hepatic arterial infusion chemotherapy or sorafenib was 7.1 and 5.5 months, respectively [26]. Furthermore, Tang et al. reported in a retrospective study consisting of 371 patients with resectable HCC with PVTT that the median OS was 10.0 and 12.3 months for surgical resection and conformal radiotherapy combined with TACE, respectively [27]. In comparison, this study demonstrated a median OS of 13.1 months in the TACE-125iodine group and 6.0 months in the TACE alone group, thus demonstrating a significant survival benefit of TACE-125iodine procedure in HCC patients complicated with PVTT in the right or left portal vein branches. This implied that TACE induced extensive intrahepatic tumor necrosis, whereas 125iodine implantation improved local tumor control in PVTT, which probably delayed PVTT progression thereby reducing the risk for tumor intrahepatic metastasis [28, 29]. This showed that TACE combined with 125iodine implantation could be used to effectively treat HCC patients with PVTT.
Similar to our results, HCC patients with PVTT that received conformal radiation therapy combined with TACE and hepatic arterial chemotherapy demonstrated response rates between 27.5%–75% with a median OS of 7–13 months [30, 31]. The advantages of implanting 125iodine seeds in the PVTT [21, 32] are as follows: (a) the radiation from seeds rendered a sustained and higher accumulative dose within the PVTT while causing minimal injury to the surrounding normal tissues, whereas serious complications like hepatitis have been reported in traditional; (b) therapy with 125iodine seeds had a low volume loss since it was not affected by respiratory movements; (c) the biological effect of the125iodine seeds was superior to three-dimensional conformal radiation since they eliminated tumor cells by maintaining them in a resting state and changing their immunophenotype thereby decreasing metastasis [30]; and this method shortened the hospitalization time of the patient thereby reducing the medical expenses when compared to conformal radiation therapy.
Similar to our data, Zhu et al. reported that HCC patients with type B PVTT of the first-order portal vein branch that underwent TACE combined with sorafenib had a median OS of 13.0 months [18]. Interestingly, all patients we analyzed underwent repeated TACE with the mean number of TACE procedures in the TACE-125iodine group being 3.1 (range, 2–6) and 3.6 (range, 2–8) in the TACE only group. Although the longer median OS in the TACE-125iodine group resulted in no significant difference in the mean number of TACE procedures between the groups (P=0.658), we observed that 125iodine implantation controlled PVTT more effectively and reduced intrahepatic metastasis. In addition, decreased intrahepatic metastasis reduced the need for the TACE procedure during the same period. Moreover, total bilirubin levels increased 4 weeks after 125iodine implantation and stabilized after 8 weeks indicating that 125iodine seeds beneficially impacted the small bile duct, which is proximal to the portal vein. Also, radiological cholangitis was mild and patients recovered without intervention.
Univariate and multivariate analysis showed that treatment method was the only independent pretreatment prognostic factor of OS. This implied that TACE combined with 125iodine seed implantation could be an effective and economical treatment option for HCC patients with PVTT in the right and left portal vein branches, especially for those who could not afford sorafenib. CT-guided 125iodine implantation was well tolerated generally with the most common adverse events being puncture site pain, seed transmigration, and a small degree of subcapsular hemorrhage that were manageable. Also, radiation-induced toxicities that are generally observed with external radiation such as loss of appetite, nausea, duodenal ulcer, hematologic abnormality, and gastrointestinal bleeding were not found [26–29]. Puncture site pain disappeared one or two days after the procedure and severe pain was treated orally by analgesic drug. Seed transmigration to the normal liver parenchyma resulted in only mild liver injury and was not addressed. The small degree of subcapsular hemorrhage that was detected on the CT scan was subsequently treated with abdominal bandage and intravenous hemostatic. Overall, severe adverse events were not observed in this study.
There are several limitations in the current study. First, this study was retrospective and therapeutic options (TACE-125iodine vs. TACE alone) in patients with advanced HCC with PVTT were individually determined on the basis of the attending physician’s preference, which likely led to selection bias within the patient population. However, the bias was limited by choosing similar baseline characteristics between the two groups [18]. Second, the sample size in this study was small and from a single center thereby probably introducing inherent bias. Thus, large prospective and multi-center studies are necessary to evaluate the efficacy of TACE-125iodine treatment in HCC patients with PVTT.
In conclusion, our study shows that TACE-125iodine procedure in unresectable HCC patients with PVTT enhances survival with minimal adverse events and is more affordable than sorafenib.
MATERIALS AND METHODS
Study design and patient selection
We reviewed the electronic medical records of 137 patients with unresectable HCC and PVTT that underwent TACE only or TACE125iodine procedure at Henan Cancer Hospital of China from January 2009 to December 2011. This study was approved by the ethics committee of our institution. The retrospective analysis of data was approved by the institutional review board. Before the patients underwent treatment, the TACE only and TACE-125iodine treatment strategies were introduced to them by the attending physicians (YQJ and GX, who introduce the two treatment methods) and the final treatment strategy was decided by the patients. If the patients chose the TACE-125iodine method, CT-guided 125iodine (CIAE-6711; Chinese Atomic Energy Science Institution, Beijing) was implanted (4.8-mm long × 0.8-mm wide) in the PVTT 4–7 days after the first TACE session. HCC was diagnosed based on non-invasive criteria in accordance with the guidelines of the European Association for the Study of Liver and American Association for the Study of Liver Disease [22]. The presence of PVTT was confirmed if a low-attenuation intraluminal mass was observed expanding the portal vein or if filling defects were detected in the portal vein branches by three-phase dynamic CT [23].
The inclusion criteria for patients in this study were as follows: (a) age between 18 and 75 years, (b) Eastern Cooperative Oncology Group performance status 0–2, (c) Child-Pugh class A or B liver disease, and (d) presence of PVTT in the right or left portal vein on CT images. Patients were excluded from this study if they (a) had main portal vein obstruction and Child-Pugh class B or C liver disease; (b) had undergone other surgery, ablation treatment, sorafenib therapy, systemic chemotherapy, intra-arterial chemoinfusion, or TACE; (c) had serious medical co-morbidities; or (d) had a history of malignant tumors in addition to HCC. The requirement to obtain informed consent was waived.
Classification of PVTT
We classified the types of PVTT into three subgroups based on a previous report [18]: (a) Type A was defined as PVTT in the main portal vein; (b) Type B was defined as PVTT in the first-order portal vein branch (the right or left portal vein); (c) Type C was defined as PVTT in the second- or lower-order portal vein branches. All patients with type B PVTT were included in the current study.
TACE procedure
TACE was performed using a 5-Fr RH catheter or microcatheter (Terumo, Tokyo, Japan) as selectively as possible based on the tumor distribution. Initially, an emulsion of 2–20ml lipiodol (Ultrafluide, Guerbet, France) and 20–40 mg doxorubicin hydrochloride was administered into the feeder vessels. The dosages of lipiodol and doxorubicin were determined according to tumor size, vascularity, presence of arterioportal shunt, and the status of liver function. Next, gelatin sponge particles were administered into the feeder vessels until stasis of arterial flow was achieved. In patients with an arterioportal shunt, embolization with polyvinyl alcohol particles (Polyvinyl Alcohol Foam Embolization Particles; Cook Medical Inc, Bloomington, IN, USA) was performed to occlude the shunt.
125iodine implantation procedure
In the TACE-125iodine group, CT-guided 125iodine implantation was performed in the PVTT, 4–7 days after the first TACE session. Before implantation, the volume and shape of each PVTT was obtained by CT scanning (Figure 3, Figure 4 and Figure 5) and used to calculate the peripheral dosage. The formula dosage, number, spatial distribution, intensity of radioactivity, and matched peripheral dosage of seeds were then calculated by the treatment planning system (TPS; FTT Technology Ltd. Co, Beijing, China; Figure 3 and Figure 4). The 125iodine seeds were implanted under CT guidance in different levels and locations of the portal vein tumor thrombosis. During the procedure, 125iodine seeds were implanted into the cancerous embolus 5mm apart along the length and 10mm apart along the width of the PVTT. After the procedure, the needle was retrieved, and the puncture site compressed for hemostasis. All patients underwent a hepatoprotection treatment after seed implantation and before discharge from the hospital.
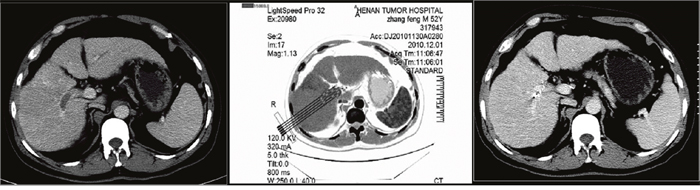
Figure 3: A 43-year-old man with hepatocellular carcinoma complicated with portal vein tumor thrombus in the right branch. Enhanced computed tomography showed the portal vein tumor thrombus originated from the right branch of the portal vein. The image prior to iodine seed implantation showed the spatial distribution of seeds according to the treatment planning system. Computed tomography demonstrated that the portal vein tumor thrombus decreased in size and that the portal vein was recanalized two months after seed implantation.
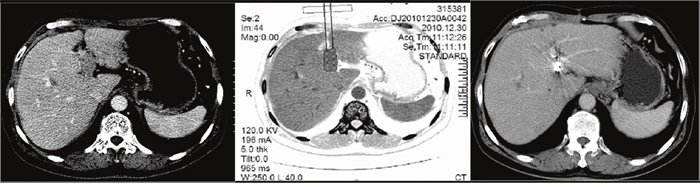
Figure 4: A 65-year-old man with hepatocellular carcinoma complicated with portal vein tumor thrombus in the left branch. Enhanced computed tomography showed the thrombus originated from the left branch of the portal vein. The image prior to iodine seed implantation showed the spatial distribution of seeds according to the treatment planning system. Computed tomography demonstrated that the portal vein tumor thrombus decreased in size and that the portal vein was recanalized two months after seed implantation.
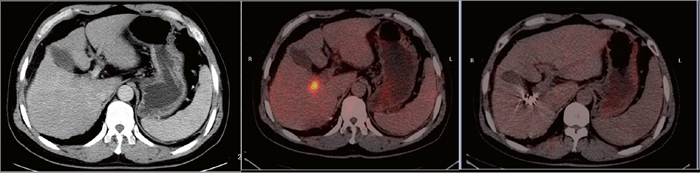
Figure 5: A 45-year-old man with hepatocellular carcinoma complicated with portal vein tumor thrombus in the right branch. Enhanced computed tomography showed the thrombus originated from the right branch of the portal vein. Positron emission tomography-computed tomography demonstrated increased fluorodeoxyglucose uptake in the right branch of the portal vein. Positron emission tomography-computed tomography demonstrated no fluorodeoxyglucose uptake in the portal vein tumor thrombus two months after seed implantation.
Follow-up and repeated TACE or 125iodine implantation
All patients who underwent treatment for HCC at our institution were required to undergo follow-up. Each follow-up session included a detailed history and physical examination, laboratory tests, and abdominal contrast material—enhanced three-phase dynamic spiral CT or magnetic resonance (MR) imaging. Laboratory tests included hematological and biochemical analyses, including complete blood cell count; prothrombin time; and α-fetoprotein, aspartate aminotransferase, alanine aminotransferase, total bilirubin, serum albumin, and creatinine levels. All patients were followed up at 4-week intervals after TACE. Patients with an intrahepatic residual viable tumor or recurrent tumor on CT or MR images underwent repeated TACE if the Child-Pugh status remained class A or B. In addition, if residual viable or recurrent PVTT was detected, 125iodine seed implantation was repeated. Treatment was terminated if the patient could not tolerate the procedure because of a decline in clinical status, loss to follow-up, or death.
Patient assessments
The clinical, laboratory, and radiologic records were reviewed. Adverse events of TACE and 125iodine implantation were reported according to National Cancer Institute Common Terminology Criteria for Adverse Events, version 3.0 [24]. In the TACE-125iodine group, 125iodine seed implantation-related adverse events were monitored until the end of seed implantation. In both groups, adverse events that occurred within 4 weeks after TACE were recorded. In addition, liver function tests that were performed 4 weeks after the first 125iodine implantation session were used to evaluate treatment toxicity to the liver. Since symptoms of post-embolization syndrome (i.e., abdominal pain, fever without any infection focus, nausea, and vomiting) were expected, they were not documented separately. We compared median overall survival (OS) between TACE-125iodine and TACE only patients. OS was defined as the time from the first TACE procedure until death or the last follow-up.
Statistical analyses
All statistical analyses were performed using SPSS version 22.0 (SPSS, Chicago, IL, USA). To determine significant differences between the two groups, Student’s t-test, χ2 test, and the Fisher exact test were used. Kaplan-Meier survival curves were constructed for both groups and evaluated. Univariate analyses were performed using the log rank test. Multivariate analyses was conducted using the Cox proportional hazard regression model on variables with a P value < 0.10 in the univariate analyses. The Wilcoxon signed-rank test was used to evaluate the differences in liver function test values before and after treatment. Two tailed statistical tests were performed and P<0.05 was considered significant.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
GRANT SUPPORT
This study was supported by grants from the National Natural Science Foundation of China [Number U1504816].
REFERENCES
1. Zhang Y, Fan W, Zhu K, Lu L, Fu S, Huang J, Wang Y, Yang J, Huang Y, Yao W, Li J. Sorafenib continuation or discontinuation in patients with unresectable hepatocellular carcinoma after a complete response. Oncotarget. 2015; 6:24550-9. doi: 10.18632/oncotarget.4076.
2. Greten TF, Korangy F, Manns MP, Malek NP. Molecular therapy for the treatment of hepatocellular carcinoma. Br J Cancer. 2009; 100:19-23. doi: 10.1038/sj.bjc.6604784
3. Nakashima T, Okuda K, Kojiro M, Jimi A, Yamaguchi R, Sakamoto K, Ikari T. Pathology of hepatocellular carcinoma in Japan. 232 Consecutive cases autopsied in ten years. Cancer, 1983; 51:863-77.
4. Lau WY. Management of hepatocellular carcinoma. J R Coll Surg Edinb. 2002; 47:389-399.
5. Lai EC, Lau WY. The continuing challenge of hepatic cancer in Asia. Surgeon. 2005; 3:210-215.
6. Zhang YF, Le Y, Wei W, Zou RH, Wang JH, OuYang HY, Xiao CZ, Zhong XP, Shi M, Guo RP. Optimal surgical strategy for hepatocellular carcinoma with portal vein tumor thrombus: A propensity score analysis. Oncotarget. 2016; 7:38845-38856. doi: 10.18632/oncotarget.8642.
7. Hu HT, Kim JH, Lee LS, Kim KA, Ko GY, Yoon HK, Sung KB, Gwon DI, Shin JH, Song HY. Chemoembolization for hepatocellular carcinoma: multivariate analysis of predicting factors for tumor response and survival in a 362-patient cohort. J Vasc Interv Radiol. 2011; 22:917-923. doi: 10.1016/j.jvir.2011.03.005.
8. Zhang XB, Wang JH, Yan ZP, Qian S, Du SS, Zeng ZC. Hepatocellular carcinoma with main portal vein tumor thrombus: treatment with 3-dimensional conformal radiotherapy after portal vein stenting and transarterial chemoembolization. Cancer. 2009; 115:1245-1252. doi: 10.1002/cncr.24139.
9. Omata M, Lesmana LA, Tateishi R, Chen PJ, Lin SM, Yoshida H, Kudo M, Lee JM, Choi BI, Poon RT, Shiina S, Cheng AL, Jia JD, et al. Asian Pacific Association for the Study of the Liver consensus recommendations on hepatocellular carcinoma. Hepatol Int. 2010; 4:439-474. doi: 10.1007/s12072-010-9165-7.
10. Forner A, Reig ME, de Lope CR, Bruix J. Current strategy for staging and treatment: the BCLC update and future prospects. Semin Liver Dis. 2010; 30:61-74. doi: 10.1055/s-0030-1247133.
11. Verslype C, Rosmorduc O, Rougier P; ESMO Guidelines Working Group. Hepatocellular carcinoma: ESMO-ESDO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2012; 23:vii41-48. doi: 10.1093/annonc/mds225
12. Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S, Kim JS, Luo R, Feng J, Ye S, Yang TS, Xu J, Sun Y, Liang H, et al. Efficacy and safety of sorafenib in patients in the double-blind, placebo-controlled trial. Lancet Oncol. 2009; 10:25-34. doi: 10.1016/S1470-2045(08)70285-7.
13. Chen CS, Li FK, Guo CY, Xiao JC, Hu HT, Cheng HT, Zheng L, Zong DW, Ma JL, Jiang L, Li HL. Tumor vascularity and lipiodol deposition as early radiological markers for predicting risk of disease progression in patients with unresectable hepatocellular carcinoma after transarterial chemoembolization. Oncotarget. 2016; 7:7241-7252. doi: 10.18632/oncotarget.6892.
14. Luo J, Guo RP, Lai EC, Zhang YJ, Lau WY, Chen MS, Shi M. Transarterial chemoembolization for unresectable hepatocellular carcinoma with portal vein tumor thrombosis: a prospective comparative study. Ann Surg Oncol. 2011; 18:413-20. doi: 10.1245/s10434-010-1321-8.
15. Xue TC, Xie XY, Zhang L, Yin X, Zhang BH, Ren ZG. Transarterial chemoembolization for hepatocellular carcinoma with portal vein tumor thrombus: a meta-analysis. BMC Gastroenterol. 2013; 13:60. doi: 10.1186/1471-230X-13-60.
16. Zhao Y, Wang WJ, Guan S, Li HL, Xu RC, Wu JB, Liu JS, Li HP, Bai W, Yin ZX, Fan DM, Zhang ZL, Han GH. Sorafenib combined with transarterial chemoembolization for the treatment of advanced hepatocellular carcinoma: a large-scale multicenter study of 222 patients. Ann Oncol. 2013; 24:1786-1792. doi: 10.1093/annonc/mdt072
17. Ha Y, Lee D, Shim JH, Lim YS, Lee HC, Chung YH, Lee YS, Park SR, Ryu MH, Ryoo BY, Kang YK, Kim KM. Role of transarterial chemoembolization in relation with sorafenib for patients with advanced hepatocellular carcinoma. Oncotarget. 2016; 7:74303-74313. doi: 10.18632/oncotarget.11030.
18. Zhu K1, Chen J, Lai L, Meng X, Zhou B, Huang W, Cai M, Shan H. Hepatocellular carcinoma with portal vein tumor thrombus: treatment with transarterial chemoembolization combined with sorafenib--a retrospective controlled study. Radiology. 2014; 272:284-293. doi: 10.1148/radiol.14131946.
19. Yang M, Fang Z, Yan Z, Luo J, Liu L, Zhang W, Wu L, Ma J, Yang Q, Liu Q. Transarterial chemoembolisation (TACE) combined with endovascular implantation of an iodine-125 seed strand for the treatment of hepatocellular carcinoma with portal vein tumour thrombosis versus TACE alone: a two-arm, randomised clinical trial. J Cancer Res Clin Oncol. 2014; 140:211-219. doi: 10.1007/s00432-013-1568-0.
20. Zhang L, Mu W, Hu CF, Huang XQ. Treatment of portal vein tumor thrombus using 125Iodine seed implantation brachytherapy. World J Gastroenterol. 2010; 16:4876-4879.
21. Zhang FJ, Li CX, Jiao DC, Zhang NH, Wu PH, Duan GF, Wu YX. CT guided 125iodine seed implantation for portal vein tumor thrombus in primary hepatocellular carcinoma. Chin Med J (Engl). 2008; 121:2410-2414.
22. Bruix J, Sherman M. Practice Guidelines Committee, American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma. Hepatology. 2005; 42:1208-1236. doi: 10.1002/hep.20933
23. Okuda K, Musha H, Yoshida T, Kanda Y, Yamazaki T. Demonstration of growing casts of hepatocellular carcinoma in the portal vein by celiac angiography: the thread and streaks sign. Radiology 1975; 117:303-309. doi: 10.1148/117.2.303
24. National Cancer Institute. Common terminology criteria for adverse events, version3.0. http://ctep.cancer.gov/reporting/ctc.html. Published August 9, 2006. Accessed June 18, 2009.
25. Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010; 30:52-60. doi: 10.1055/s-0030-1247132.
26. Song DS, Bae SH, Song MJ, Lee SW, Kim HY, Lee YJ, Oh JS, Chun HJ, Lee HG, Choi JY, Yoon SK. Hepatic arterial infusion chemotherapy in hepatocellular carcinoma with portal vein tumor thrombosis. World J Gastroenterol. 2013; 19:4679-4688. doi: 10.3748/wjg.v19.i29.4679.
27. Tang QH, Li AJ, Yang GM, Lai EC, Zhou WP, Jiang ZH, Lau WY, Wu MC. Surgical resection versus conformal radiotherapy combined with TACE for resectable hepatocellular carcinoma with portal vein tumor thrombus: a comparative study. World J Surg. 2013; 37:1362-1370. doi: 10.1007/s00268-013-1969-x.
28. Nakagawa K, Yamashita H, Shiraishi K, Nakamura N, Tago M, Igaki H, Hosoi Y, Shiina S, Omata M, Makuuchi M, Ohtomo K. Radiation therapy for portal venous invasion by hepatocellular carcinoma. World J Gastroenterol. 2005; 11:7237-7241.
29. Kim JY, Chung SM, Choi BO, Kay CS. Hepatocellular carcinoma with portal vein tumor thrombosis: Improved treatment outcomes with external beam radiation therapy. Hepatol Res. 2011; 41:813-824. doi: 10.1111/j.1872-034X.2011.00826.x.
30. Ling CC. Permanent implants using Au-198, Pd-103 and I-125: radiobiological considerations based on the linear quadratic model. Int J Radiat Oncol Biol Phys. 1992; 23:81-87.
31. Oh D, Lim DH, Park HC, Paik SW, Koh KC, Lee JH, Choi MS, Yoo BC, Lim HK, Lee WJ, Rhim H, Shin SW, Park KB. Early three-dimensional conformal radiotherapy for patients with unresectable hepatocellular carcinoma after incomplete transcatheter arterial chemoembolization: a prospective evaluation of efficacy and toxicity. Am J Clin Oncol. 2010; 33:370-375. doi: 10.1097/COC.0b013e3181b0c298.
32. Jiao D, Wu G, Ren J, Han X. Radiofrequency ablation versus 125I-seed brachytherapy for painful metastases involving the bone. Oncotarget. 2016; 7:87523-87531. doi: 10.18632/oncotarget.11983.