
INTRODUCTION
Glaucoma is the second-leading cause of irreversible blindness in the world [1]. Data has been estimated that over 11.1 million people will be bilaterally blind from primary glaucoma by 2020 [1]. Glaucoma is characterized by degeneration of the optic nerve, and is usually associated with increased intraocular pressure [2]. The main types of glaucoma include primary open-angle glaucoma (POAG) and primary angle closure glaucoma (PACG). To date, the main pathogenesis for disease progression in glaucoma is still poorly understood. Studies suggested that various risk factors of glaucoma included age, elevated intraocular pressure (IOP), variable susceptibility of the optic nerve, vascular factors, diabetes, myopia, a positive family history and cigarette smoking [3]. Genetic factors also have been reported to play a vital role in the pathogenesis of glaucoma [4, 5]. Previous linkage-based studies demonstrated several genes were associated with glaucoma, including myocilin, CYP1B1, optineurin, and WDR36 [6–8]. Recent genome-wide association studies (GWASs) have identified several genetic variants associated with glaucoma [9], including cyclin-dependent kinase Inhibitor-2B (CDKN2B) gene.
CDKN2B has been identified to play an important role in G1 progression of the cell cycle [10]. Animal studies demonstrated that elevated IOP is associated with overexpression of CDKN2B, which leads to disruption in cell cycle causing abnormal cell proliferation [11]. GWAS studies for glaucoma showed direct association of CDKN2B region of 9p21 locus with glaucoma, identifying its significance as a risk factor [12, 13]. A host of studies [12-26] investigated the association between CDKN2B gene rs1063192 polymorphism and glaucoma susceptibility, but with conflicting findings. However, these studies were conflicting and inconclusive due to clinical heterogeneity, different ethnic populations, and small sample sizes. Therefore, we performed a comprehensive meta-analysis to clarify the possible association between CDKN2B gene rs1063192 polymorphism and glaucoma risk.
RESULTS
Characteristics of the included studies
We yielded a total of 76 citations the by searches of the PubMed and Embase databases and manual searching. 43 citations were removed after removing duplicates and screening the titles and abstracts. 33 citations were selected for further full text review. 19 citations (3 citations did not conform to the inclusion criteria; 6 investigated other polymorphisms; 5 did not provide detailed genotyping data; 1 overlapped with previous study; 3 were reviews; and 1 was not case-control study) were excluded after serious review. 14 eligible studies [12–17, 19–26] (11,316 cases and 24,055 controls) in this meta-analysis finally. Selection for eligible studies included in this meta-analysis was presented in Figure 1. The characteristics of the individual studies included in the meta-analysis are summarized in Table 1. The Newcastle-Ottawa Scale (NOS) scores of all included studies ranged from 6 to 7 stars, suggesting that these studies were of high methodological quality.
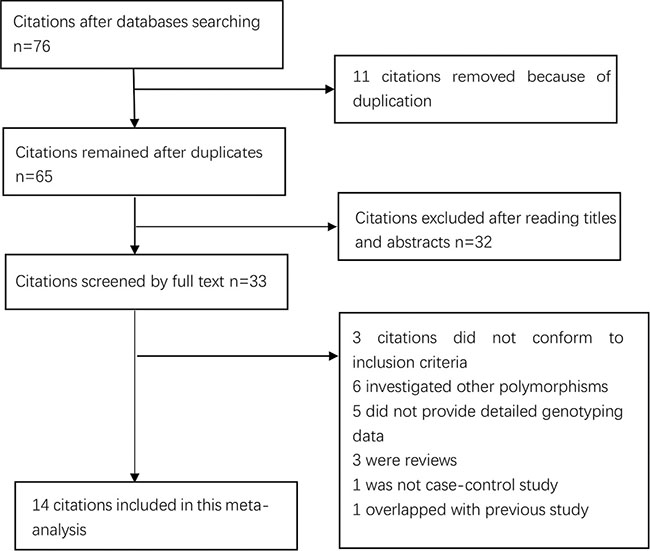
Figure 1: Selection for eligible publications included in this meta-analysis.
Table 1: Characteristics of included studies
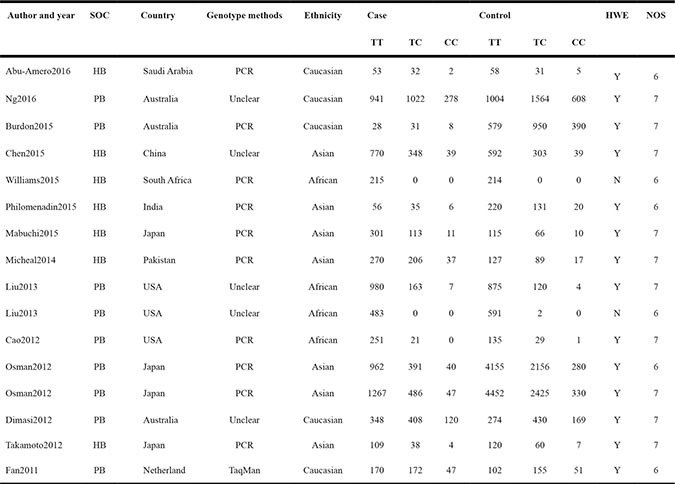
SOC, source of controls; PB, population-based controls; HB, hospital-based controls; HWE, Hardy–Weinberg Equilibrium; NOS, Newcastle-Ottawa Scale.
Meta-analysis of CDKN2B gene rs1063192 polymorphism with glaucoma risk
A summary of association between CDKN2B gene rs1063192 polymorphism with glaucoma risk is provided in Tables 2 and 3. In the overall analysis, we detected a significant association between CDKN2B gene rs1063192 polymorphism with the decreased risk of glaucoma (CC vs. TT: OR, 0.55; 95% CI, 0.49–0.61, P < 0.001, Figure 2). Stratification by ethnicity indicated that rs1063192 polymorphism was also significantly associated with a decreased risk of glaucoma among Caucasians and Asians (C vs. T, Figure 3). Similar result was also replicated among Africans in the allele model (C vs. T, Figure 3). Stratification analysis by type of glaucoma suggested that rs1063192 polymorphism was a protective factor of POAG and non-POAG (TT vs. CT + CC, Figure 4). Stratification by source of controls (SOCs) revealed an association between rs1063192 polymorphism and glaucoma in groups of population-based controls.
Table 2: Meta-analysis of association between CDKN2B rs1063192 polymorphism and the risk of glaucoma
Comparison |
OR(95%CI) |
P-value |
P for heterogeneity |
I2 (%) |
Model |
|---|---|---|---|---|---|
C vs. T |
0.79 (0.72,0.87) |
< 0.001 |
< 0.001 |
68.2 |
Random |
CC + TC vs. TT |
0.76 (0.68,0.85) |
< 0.001 |
< 0.001 |
69.2 |
Random |
CC vs. TT + TC |
0.64 (0.58,0.71) |
< 0.001 |
0.730 |
0.0 |
Fixed |
CC vs. TT |
0.55 (0.49,0.61) |
< 0.001 |
0.286 |
15.3 |
Fixed |
TC vs. TT |
0.94 (0.82,1.07) |
< 0.001 |
0.002 |
59.3 |
Random |
*Bold values are statistically significant (P < 0.05).
Table 3: Summary of the subgroup analyses in this meta-analysis
Comparison |
Category |
Category |
Studies |
OR (95% CI) |
P-value |
P for heterogeneity |
|---|---|---|---|---|---|---|
C vs. T |
Ethnicity |
Caucasian |
5 |
0.71 (0.67,0.72) |
< 0.001 |
0.724 |
Asian |
7 |
0.81 (0.72,0.91) |
< 0.001 |
0.013 |
||
African |
3 |
0.79 (0.72,0.87) |
0.404 |
0.001 |
||
Type of glaucoma |
POAG |
12 |
0.78 (0.70,0.87) |
< 0.001 |
< 0.001 |
|
Non-POAG |
3 |
0.81 (0.63,1.04) |
0.096 |
0.037 |
||
SOC |
HB |
6 |
0.88 (0.75,1.02) |
0.080 |
0.174 |
|
PB |
9 |
0.75 (0.67,0.83) |
< 0.001 |
0.001 |
||
CC + TC vs. TT |
Ethnicity |
Caucasian |
5 |
0.66 (0.60,0.72) |
< 0.001 |
0.575 |
Asian |
7 |
0.79 (0.69,0.90) |
< 0.001 |
0.026 |
||
African |
3 |
0.63 (0.22,1.84) |
0.402 |
0.001 |
||
Type of glaucoma |
POAG |
12 |
0.75 (0.66,0.86) |
< 0.001 |
< 0.001 |
|
Non-POAG |
3 |
0.78 (0.56,1.09) |
0.143 |
0.038 |
||
SOC |
HB |
6 |
0.87 (0.73,1.03) |
< 0.001 |
0.204 |
|
PB |
9 |
0.71 (0.62,0.82) |
0.107 |
< 0.001 |
||
CC vs.TC + TT |
Ethnicity |
Caucasian |
5 |
0.62 (0.54,0.70) |
< 0.001 |
0.898 |
Asian |
7 |
0.67 (0.56,0.80) |
< 0.001 |
0.493 |
||
African |
2 |
1.12 (0.38,3.34) |
0.838 |
0.247 |
||
Type of glaucoma |
POAG |
11 |
0.63 (0.56,0.70) |
< 0.001 |
0.719 |
|
Non-POAG |
3 |
0.69 (0.55,0.86) |
0.001 |
0.375 |
||
SOC |
HB |
6 |
0.80 (0.59,1.08) |
0.148 |
0.701 |
|
PB |
8 |
0.62 (0.55,0.69) |
< 0.001 |
0.779 |
||
CC vs.TT |
Ethnicity |
Caucasian |
5 |
0.51 (0.44,0.58) |
< 0.001 |
0.907 |
Asian |
7 |
0.62 (0.51,0.74) |
< 0.001 |
0.258 |
||
African |
2 |
1.13 (0.38,3.35) |
0.831 |
0.216 |
||
Type of glaucoma |
POAG |
11 |
0.55 (0.48,0.63) |
< 0.001 |
0.371 |
|
Non-POAG |
3 |
0.63 (0.41,0.96) |
0.033 |
0.142 |
||
SOC |
HB |
6 |
0.78 (0.58,1.06) |
0.108 |
0.560 |
|
PB |
8 |
0.52 (0.47,0.59) |
< 0.001 |
0.581 |
||
TC vs.TT |
Ethnicity |
Caucasian |
5 |
0.71 (0.65,0.78) |
< 0.001 |
0.615 |
Asian |
7 |
0.80 (0.71,0.90) |
< 0.001 |
0.081 |
||
African |
3 |
0.64 (0.23,1.81) |
0.404 |
0.002 |
||
Type of glaucoma |
POAG |
12 |
0.78 (0.69,0.88) |
< 0.001 |
0.002 |
|
Non-POAG |
3 |
0.83 (0.63,1.10) |
0.190 |
0.122 |
||
SOC |
HB |
6 |
0.89 (0.76,1.04) |
0.138 |
0.294 |
|
PB |
9 |
0.75 (0.66,0.85) |
< 0.001 |
0.004 |
SOC, source of control; PB, population-based controls; HB, hospital-based controls; POAG: Primary Open-Angle Glaucoma.
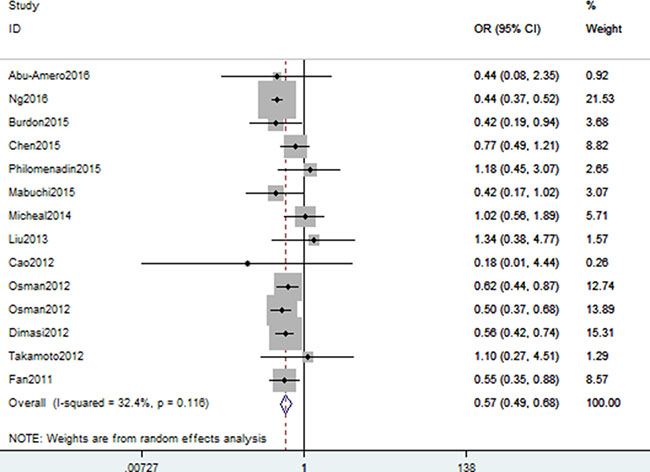
Figure 2: Forest plot shows odds ratio for the associations between rs1063192 polymorphism and glaucoma risk (CC vs. TT).
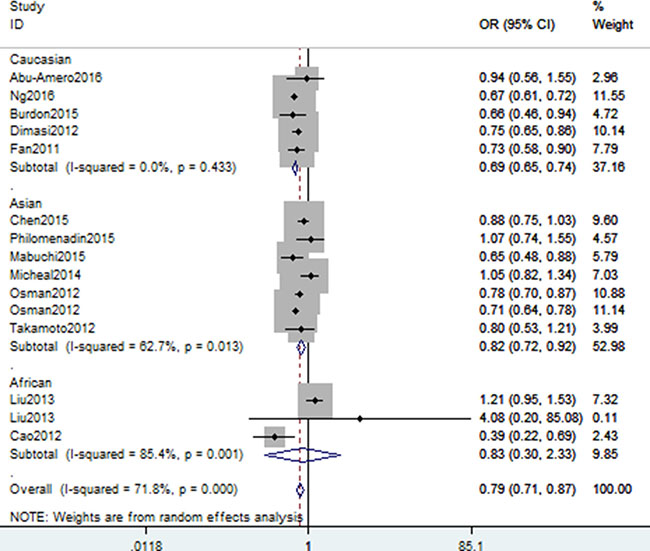
Figure 3: Stratification analysis of ethnicity shows odds ratio for the association between rs1063192 polymorphism and glaucoma risk (C vs. T).
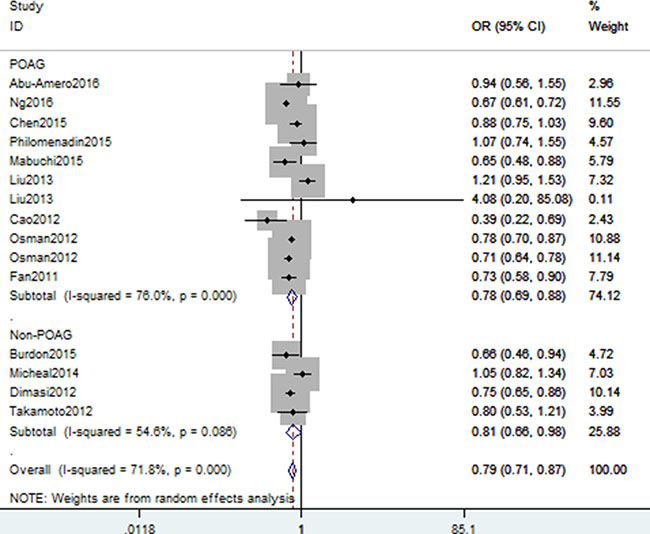
Figure 4: Stratification analysis of type of glaucoma between rs1063192 polymorphism and glaucoma risk (TT vs. CT + CC).
We assessed sensitivity by omitting each study once at a time in every genetic model for rs1063192 polymorphism. The pooled ORs for the effects of the single nucleotide polymorphism (SNP) on the risk for glaucoma risk indicated that our data was stable and trustworthy(C vs. T, Figure 5). Both Egger’s and Begg’s tests (CC vs. TT, Figure 6) were used to evaluated the publication bias of this meta-analysis. Our data showed no evidence of publication bias affecting the meta-analysis results. (data not shown).
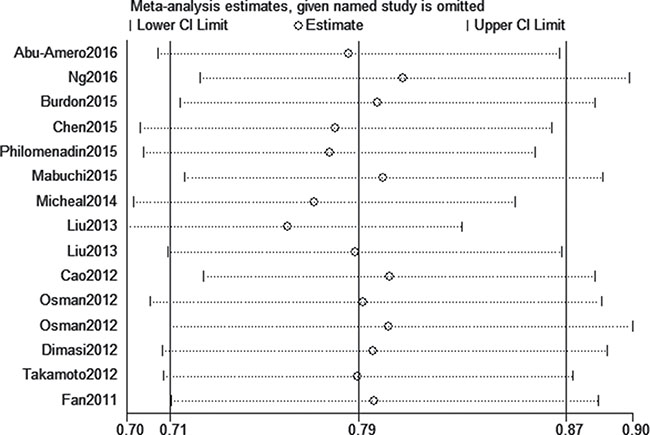
Figure 5: Sensitivity analysis for rs1063192 polymorphism and glaucoma risk (C vs. T).
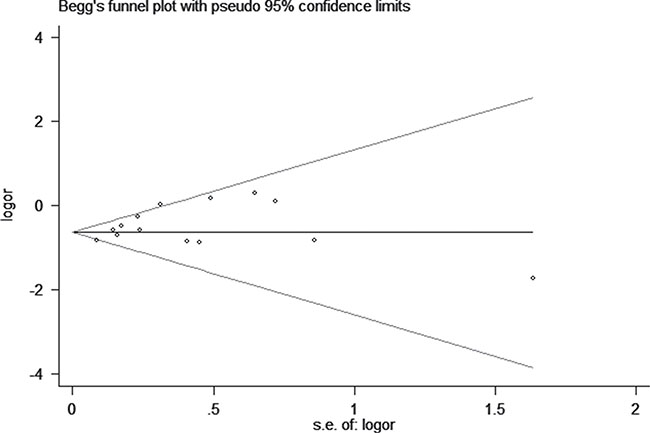
Figure 6: Begg’s tests between rs1063192 polymorphism and glaucoma risk (CC vs. TT)
DISCUSSION
In this meta-analysis, our data indicated that CDKN2B gene rs1063192 polymorphism with the decreased risk of glaucoma. Stratification analysis by ethnicity found that rs1063192 polymorphism decreased the risk of glaucoma among Caucasians, Asians and Africans. Stratification analysis by type of glaucoma revealed that rs1063192 polymorphism was associated with a decreased risk of POAG and non-POAG.
Genes at the 9p21 locus, including CDKN2B, are strong candidates for POAG risk. CDKN2B gene plays a vital role in cell cycle, development and function of ophthalmic disorders [27]. Several GWASs among different ethnic groups provided strong evidence that gene variants at the CDKN2B locus of 9p21 are a crucial risk factor in the development of POAG [12, 23, 28, 29]. Recently, a host of studies [12–26] explored the association between CDKN2B gene rs1063192 polymorphism and glaucoma risk. However, these studies obtained conflicting results. The limitations of these studies [12–26] including clinical heterogeneity, different ethnic populations, and small sample sizes may contribute to the disaccords. Although association studies provide a powerful means of identifying genetic factors underlying glaucoma, most reported association studies lack sufficient statistical power. In such cases, meta-analysis can be used as an alternative. Therefore, we conducted this comprehensive meta-analysis to demonstrate the association between CDKN2B gene rs1063192 polymorphism and glaucoma susceptibility. To the best of our knowledge, this is the first meta-analysis to explore the relationship between this SNP and glaucoma risk.
In this meta-analysis, we combined data from included studies to evaluate genetic association between CDKN2B gene rs1063192 polymorphism and glaucoma. Our results showed a significant association between this SNP and glaucoma. Meta-analysis showed a significant association between rs1063192 polymorphism and glaucoma risk in Caucasians, Asians, and Africans, indicating that there was no significant ethnic differences about this SNP. It is of note that we only found the positive finding among Africans in the allele model, but the other four genetic models failed to replicate this association. The result of stratification analysis among Africans should be interpreted with caution, because the racial stratification of CDKN2B gene rs1063192 polymorphism and glaucoma regarding Africans included only three studies, which is insufficient to provide conclusive evidence. Thus, further studies using larger numbers of subjects are required. As for the subgroup analysis by type of glaucoma, we found rs1063192 polymorphism was associated with a decreased risk of POAG and non-POAG patients. Although the clinical heterogeneity of POAG and non-POAG is evident, meta-analysis did not find any different results between them. It is noteworthy that this meta-analysis only included 3 studies with limited sample size for non-POAG. Hence, we could exclude the likelihood of false-positive associations.
We believe our meta-analysis has some strengths. One, we included 14 studies with 11,316 cases and 24,055 controls in this study and the sample size of this meta-analysis was large. Two, sensitivity analysis provided evidence that our data about CDKN2B gene rs1063192 polymorphism were trustworthy and robust. Three, the power analysis indicated that our study had a power of 99.0% to detect the effect of rs1063192 polymorphism on glaucoma susceptibility, assuming an OR of 0.76.
However, this meta-analysis has some limitations that require further consideration. First, due to limited data, we could not perform further stratification analyses of other potential factors, such as age and gender. Second, our results were based on unadjusted estimates for confounding factors, which might have affected the final conclusions. Third, we could not assess potential gene-gene and gene-environment interactions because of the lack of relevant data. Fourth, the ethnicity-specific meta-analysis included data from Caucasians, Asians, and Africans, and thus, our findings are only applicable to these ethnic groups. Fifth, some unpublished studies may have been missed, although our data indicated no evident publication bias. Sixth, CDKN2B gene rs1063192 polymorphism would be not enough to explain the associations between CDKN2B gene and glaucoma risk. Seventh, the heterogeneity of this meta-analysis was high in some genetic models. Last but not least, the sample size of stratification analysis was limited in some ethnicities.
In conclusion, this meta-analysis demonstrates that CDKN2B gene rs1063192 polymorphism is significantly associated with a decreased risk of glaucoma. Larger scale studies of populations with different ethnicities are necessary to explore the roles played by this SNP of CDKN2B gene during the pathogenesis of glaucoma.
MATERIALS AND METHODS
Identification of eligible studies and data extraction
A literature search was performed in the databases of PubMed and Embase to identify studies through December 8, 2016. The following words were used: “tumor necrosis factor alpha inducible protein 3,” ‘‘glaucoma,’’ ‘‘primary open angle glaucoma,’’ ‘‘POAG,’’ ‘‘primary angle closure glaucoma,’’ ‘‘polymorphism,’’ ‘‘PACG’’ “cyclin-dependent kinase Inhibitor-2B” and ‘‘CDKN2B’’. No restrictions were placed on the search. Hand screening was conducted in order to identify additional studies. The identified studies conformed to the following criteria: (1) studies that evaluated the association between glaucoma and CDKN2B gene rs1063192 polymorphism, (2) studied on human beings, (3) study provided sufficient data to calculate the odds ratios (ORs) and 95% confidence intervals (CIs), and P value, and (4) case-control study.
The relevant data were extracted from the original articles. The extracted information from all eligible studies including: name of first author, publication year, ethnicity, and genotype numbers of cases and controls. Two reviewers independently performed the extraction of data and assessed the study quality based on the NOS [30]. Any discrepancies between the reviewers were resolved by consensus or by a third reviewer.
Statistical analysis
Statistical manipulations were performed using the Stata 11.0 software (StataCorp, College Station, TX, USA). ORs and 95%CIs were used to assess the strength of associations between CDKN2B gene rs1063192 polymorphism and glaucoma risk. Stratification analysis was carried out by ethnicity, type of glaucoma and source of controls. Cochran’s Q statistic was also used to assess within- and between study variation, and tests of heterogeneity were used to assess the null hypothesis that all studies evaluated the same effect. When a Q test indicated P < 0.1 or I2 > 50% indicated heterogeneity across studies, a random-effect model was used. Otherwise, the fixed-effects model was applied [31]. Pooled ORs were calculated for allele model, dominant model, recessive model, homozygous model, and heterozygous model. Sensitivity analyses were performed by omitting each study in turn to determine the effect on the test of heterogeneity and evaluated the stability of the overall results. We assessed the departure from the HWE in the controls using Pearson’s χ2 test. Potential publication bias was assessed by Begger’s and Egger’s linear regression test [32]; P < 0.05 was considered to indicate statistically significant. The power of this meta-analysis was calculated with a significant value of 0.05 [33].
Abbreviations
CDKN2B, cyclin-dependent kinase Inhibitor-2B; POAG, primary open-angle glaucoma; PACG, primary angle closure glaucoma; IOP, intraocular pressure; CI, confidence interval; OR, odds ratio; NOS, Newcastle-Ottawa Scale; SNP, single nucleotide polymorphism; GWAS, Genome-wide association studies.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
REFERENCES
1. Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. The British journal of ophthalmology. 2006; 90:262–267.
2. Weinreb RN, Khaw PT. Primary open-angle glaucoma. Lancet. 2004; 363:1711–1720.
3. Worley A, Grimmer-Somers K. Risk factors for glaucoma: what do they really mean? Aust J Prim Health. 2011; 17:233–239.
4. Liu Y, Allingham RR. Molecular genetics in glaucoma. Experimental eye research. 2011; 93:331–339.
5. Fan BJ, Wiggs JL. Glaucoma: genes, phenotypes, and new directions for therapy. J Clin Invest. 2010; 120:3064–3072.
6. Stone EM, Fingert JH, Alward WL, Nguyen TD, Polansky JR, Sunden SL, Nishimura D, Clark AF, Nystuen A, Nichols BE, Mackey DA, Ritch R, Kalenak JW, et al. Identification of a gene that causes primary open angle glaucoma. Science. 1997; 275:668–670.
7. Rezaie T, Child A, Hitchings R, Brice G, Miller L, Coca-Prados M, Heon E, Krupin T, Ritch R, Kreutzer D, Crick RP, Sarfarazi M. Adult-onset primary open-angle glaucoma caused by mutations in optineurin. Science. 2002; 295:1077–1079.
8. Monemi S, Spaeth G, DaSilva A, Popinchalk S, Ilitchev E, Liebmann J, Ritch R, Heon E, Crick RP, Child A, Sarfarazi M. Identification of a novel adult-onset primary open-angle glaucoma (POAG) gene on 5q22.1. Human molecular genetics. 2005; 14:725–733.
9. Burdon KP, Macgregor S, Hewitt AW, Sharma S, Chidlow G, Mills RA, Danoy P, Casson R, Viswanathan AC, Liu JZ, Landers J, Henders AK, Wood J, et al. Genome-wide association study identifies susceptibility loci for open angle glaucoma at TMCO1 and CDKN2B-AS1. Nature genetics. 2011; 43:574–578.
10. Hannon GJ, Beach D. p15INK4B is a potential effector of TGF-beta-induced cell cycle arrest. Nature. 1994; 371: 257–261.
11. Iglesias AI, Springelkamp H, van der Linde H, Severijnen LA, Amin N, Oostra B, Kockx CE, van den Hout MC, van Ijcken WF, Hofman A, Uitterlinden AG, Verdijk RM, Klaver CC, et al. Exome sequencing and functional analyses suggest that SIX6 is a gene involved in an altered proliferation-differentiation balance early in life and optic nerve degeneration at old age. Human molecular genetics. 2014; 23:1320–1332.
12. Osman W, Low SK, Takahashi A, Kubo M, Nakamura Y. A genome-wide association study in the Japanese population confirms 9p21 and 14q23 as susceptibility loci for primary open angle glaucoma. Human molecular genetics. 2012; 21:2836–2842.
13. Cao D, Jiao X, Liu X, Hennis A, Leske MC, Nemesure B, Hejtmancik JF. CDKN2B polymorphism is associated with primary open-angle glaucoma (POAG) in the Afro-Caribbean population of Barbados, West Indies. PloS one. 2012; 7:e39278.
14. Takamoto M, Kaburaki T, Mabuchi A, Araie M, Amano S, Aihara M, Tomidokoro A, Iwase A, Mabuchi F, Kashiwagi K, Shirato S, Yasuda N, Kawashima H, et al. Common variants on chromosome 9p21 are associated with normal tension glaucoma. PloS one. 2012; 7:e40107.
15. Philomenadin FS, Asokan R, N V, George R, Lingam V, Sarangapani S. Genetic association of SNPs near ATOH7, CARD10, CDKN2B, CDC7 and SIX1/SIX6 with the endophenotypes of primary open angle glaucoma in Indian population. PloS one. 2015; 10:e0119703.
16. Ng SK, Burdon KP, Fitzgerald JT, Zhou T, Fogarty R, Souzeau E, Landers J, Mills RA, Casson RJ, Ridge B, Graham SL, Hewitt AW, Mackey DA, et al. Genetic Association at the 9p21 Glaucoma Locus Contributes to Sex Bias in Normal-Tension Glaucoma. Investigative ophthalmology & visual science. 2016; 57:3416–3421.
17. Micheal S, Ayub H, Khan MI, Bakker B, Schoenmaker-Koller FE, Ali M, Akhtar F, Khan WA, Qamar R and den Hollander AI. Association of known common genetic variants with primary open angle, primary angle closure, and pseudoexfoliation glaucoma in Pakistani cohorts. Molecular vision. 2014; 20:1471–1479.
18. Mabuchi F, Sakurada Y, Kashiwagi K, Yamagata Z, Iijima H, Tsukahara S. Association between genetic variants associated with vertical cup-to-disc ratio and phenotypic features of primary open-angle glaucoma. Ophthalmology. 2012; 119:1819–1825.
19. Liu Y, Hauser MA, Akafo SK, Qin X, Miura S, Gibson JR, Wheeler J, Gaasterland DE, Challa P, Herndon LW, Ritch R, Moroi SE, Pasquale LR, et al. Investigation of known genetic risk factors for primary open angle glaucoma in two populations of African ancestry. Investigative ophthalmology & visual science. 2013; 54:6248–6254.
20. Fan BJ, Wang DY, Pasquale LR, Haines JL, Wiggs JL. Genetic variants associated with optic nerve vertical cup-to-disc ratio are risk factors for primary open angle glaucoma in a US Caucasian population. Investigative ophthalmology & visual science. 2011; 52:1788–1792.
21. Dimasi DP, Burdon KP, Hewitt AW, Fitzgerald J, Wang JJ, Healey PR, Mitchell P, Mackey DA, Craig JE. Genetic investigation into the endophenotypic status of central corneal thickness and optic disc parameters in relation to open-angle glaucoma. American journal of ophthalmology. 2012; 154:833–842.e832.
22. Chen Y, Hughes G, Chen X, Qian S, Cao W, Wang L, Wang M, Sun X. Genetic Variants Associated With Different Risks for High Tension Glaucoma and Normal Tension Glaucoma in a Chinese Population. Investigative ophthalmology & visual science. 2015; 56:2595–2600.
23. Burdon KP, Mitchell P, Lee A, Healey PR, White AJ, Rochtchina E, Thomas PB, Wang JJ, Craig JE. Association of open-angle glaucoma loci with incident glaucoma in the Blue Mountains Eye Study. American journal of ophthalmology. 2015; 159:31–36.e31.
24. Abu-Amero KK, Kondkar AA, Mousa A, Almobarak FA, Alawad A, Altuwaijri S, Sultan T, Azad TA, Al-Obeidan SA. Analysis of Cyclin-Dependent Kinase Inhibitor-2B rs1063192 Polymorphism in Saudi Patients with Primary Open-Angle Glaucoma. Genetic testing and molecular biomarkers. 2016; 20:637–641.
25. Williams SE, Carmichael TR, Allingham RR, Hauser M, Ramsay M. The genetics of POAG in black South Africans: a candidate gene association study. Scientific reports. 2015; 5:8378.
26. Mabuchi F, Sakurada Y, Kashiwagi K, Yamagata Z, Iijima H, Tsukahara S. Involvement of genetic variants associated with primary open-angle glaucoma in pathogenic mechanisms and family history of glaucoma. American journal of ophthalmology. 2015; 159:437–444.e432.
27. Janssen SF, Gorgels TG, Ramdas WD, Klaver CC, van Duijn CM, Jansonius NM, Bergen AA. The vast complexity of primary open angle glaucoma: disease genes, risks, molecular mechanisms and pathobiology. Progress in retinal and eye research. 2013; 37:31–67.
28. Li Z, Allingham RR, Nakano M, Jia L, Chen Y, Ikeda Y, Mani B, Chen LJ, Kee C, Garway-Heath DF, Sripriya S, Fuse N, Abu-Amero KK, et al. A common variant near TGFBR3 is associated with primary open angle glaucoma. Human molecular genetics. 2015; 24:3880–3892.
29. Wiggs JL, Yaspan BL, Hauser MA, Kang JH, Allingham RR, Olson LM, Abdrabou W, Fan BJ, Wang DY, Brodeur W, Budenz DL, Caprioli J, Crenshaw A, et al. Common variants at 9p21 and 8q22 are associated with increased susceptibility to optic nerve degeneration in glaucoma. PLoS genetics. 2012; 8:e1002654.
30. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010; 25:603–605.
31. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002; 21:1539–1558.
32. Peters JL, Sutton AJ, Jones DR, Abrams KR, Rushton L. Comparison of two methods to detect publication bias in meta-analysis. Jama. 2006; 295:676–680.
33. Hedges LV, Pigott TD. The power of statistical tests in meta-analysis. Psychol Methods. 2001; 6:203–217.