
INTRODUCTION
Lung carcinomas are the leading cause of cancer-related mortality worldwide [1]. Adenocarcinoma is the most common histologic type of lung cancer [2]. With the development of targeted therapy, adenocarcinoma are classified into subsets, such as epidermal growth factor receptor (EGFR)-mutated type [3, 4], anaplastic lymphoma kinase (ALK)-rearranged type [5] and ROS1-rearranged type [6]. The ROS1-rearranged non-small-cell lung carcinomas (NSCLCs) have been reported to be sensitive to the kinase inhibitor crizotinib [7].
Correlation between histology and genotype has been described in lung adenocarcinomas. For example, several studies have suggested that ALK-rearranged lung adenocarcinomas were most likely to be observed in the cases with signet-ring cells [8–11]. Boland et al found that 26% pulmonary adenocarcinoma with signet ring cell features were ALK rearrangement [8]. However, comprehensive clinical and histological characteristics of ROS1 rearrangement were not well known given the rarity of this subtype. Data describing the morphologic features of ROS1-rearranged lung adenocarcinomas are primarily based on analysis of resected primary lung tumors [12–14]. However, approximately 70% of patients are at advanced stage when diagnosed. For these patients, the small biopsies or cytological specimens are the only limited pathologic material available for diagnosis and molecular testing. It is still unclear whether the findings from prior studies are applicable to specimens from metastatic lung tumors, small biopsies or cytology specimens.
In this study, we confirmed 19 advanced patients with ROS1 rearrangement by real-time PCR and ROS1 FISH and compared their clinical features and histological characteristics with ROS1-subtype. Furthermore, we identified independent predictors for ROS1 rearrangement by multiple logistic regression analysis.
RESULTS
Clinical Characteristics of patients with ROS1-rearranged NSCLCs
Of the 516 consecutive patients from the advanced NSCLCs, ROS1 rearrangements were detected in 19 cases (3.7%) using real-time PCR, 488 cases were negative and 9 cases failed. The tissues were available for FISH in 513 of 516 cases. One lymph node biopsy and two biopsies can’t be detected by FISH because of few tumor cells and twelve cases were not interpretable. 18 cases were confirmed positive in both real-time PCR and ROS1 FISH. One lymph node biopsy was eliminated because of few tumor cells. In ROS1 FISH positive patients (n=18), a split pattern was observed in 17 tumors (94.4%), and an isolated red pattern was observed in one tumors (5.6%). One lymph node biopsy with few tumor cells and two cell blocks were not included in histological assessment. The clinical features of 16 patients with ROS1-rearranged were summarized in Table 1. ROS1-rearranged advanced NSCLCs were associated with a younger age at presentation. Patients with ROS1-rearranged tumors had an age range of 38–67 years and mean age of 50 years (compared with mean age of 59 years for patients with ROS1-wildtype tumors, P=0.001). ROS1 rearrangements were not significantly associated with sex, smoking history, drinking history and metastatic sites (Table 2).
Table 1: Clinical characteristics of patients tested in our study
N=516 |
|||
|---|---|---|---|
Mean age (range) |
58 |
(25-79) |
|
Sex |
Male |
269 |
|
Female |
247 |
||
Smoking status |
|||
never |
287 |
||
Former |
229 |
||
Gene status |
|||
EGFR mutated |
241 |
||
ALK rearranged |
26 |
||
Pan WT |
230 |
||
ROS1 rearranged |
19 |
||
Table 2: Clinicopathologic features of ROS1+ and ROS1- advanced lung adenocarcinomas
ROS1+ |
ROS1− |
P-value |
||
|---|---|---|---|---|
Age |
50 |
59 |
0.001* |
|
Sex(M:F) |
6:10 |
66:56 |
0.328 |
|
Smoking status |
0 |
10 |
67 |
0.317 |
<20 |
2 |
8 |
||
≥20 |
4 |
47 |
||
Drinking status |
NO |
11 |
91 |
0.784 |
Yes |
5 |
31 |
||
Metastatic sites |
Bone |
5 |
57 |
0.370 |
Brain |
2 |
27 |
0.333 |
|
Adrenal |
3 |
17 |
0.629 |
|
Liver |
1 |
17 |
0.323 |
|
Lung |
3 |
38 |
0.588 |
|
Extra thoracic lymph nodes |
4 |
23 |
0.151 |
|
Histomorphology |
||||
Any Lepidic pattern |
0 |
6 |
1.000 |
|
Any Acinar pattern |
4 |
49 |
0.286 |
|
Any Papillary pattern |
0 |
9 |
0.598 |
|
Any Solid pattern |
12 |
76 |
0.417 |
|
Any Micropapillary pattern |
0 |
4 |
1.000 |
|
Cribriform feature |
3 |
4 |
0.034* |
|
Extracellular mucus |
1 |
3 |
0.393 |
|
Signet-ring cells |
2 |
5 |
0.187 |
|
Psammoma body |
1 |
4 |
0.465 |
|
Hepatiod cell |
8 |
10 |
0.016* |
|
Cytological atypia |
mild atypia |
0 |
28 |
0035* |
moderate atypia |
8 |
63 |
||
severe atypia |
8 |
31 |
M: male; F: female.
* indicates parameters showing statistical significance.
Histologic Characteristics of ROS1-rearranged NSCLCs
All 16 ROS1-rearranged tumors were adenocarcinomas (Supplementary Table S1). In 5 tumors, diffuse co-expression of TTF-1 and p63 was observed, and 2 of them were also positive for CK5/6, and 4 of them were positive for p40 (Figure 1). The histologic characteristics of ROS1-rearranged NSCLCs were described in detail in Table 2. The solid growth pattern was the most commonly observed in 75% (12/16) of ROS1-rearranged tumors, followed by the acinar-pattern (25%, 4/16) (Figure 2). None of 16 cases was lepidic, papillary or micropapillary growth pattern. 66.7% cases with solid growth pattern showed hepatoid cytology (8/12) (Figure 2A–2D), which had eosinophilic cytoplasm, round nuclei and obvious nucleoli. These 8 cases were negative for antibodies Hep, AFP and Gpc3, and serum alpha-fetoprotein (AFP) were also low (0.6-2.8ng/ml). 75% cases with acinar growth pattern showed a cribriform structure (3/4) (Figure 2E–2F). 18.8% cases were found to have abundant extracellular mucus or signet-ring cells (3/16). Only one case with solid growth pattern showed psammomatous calcifications.
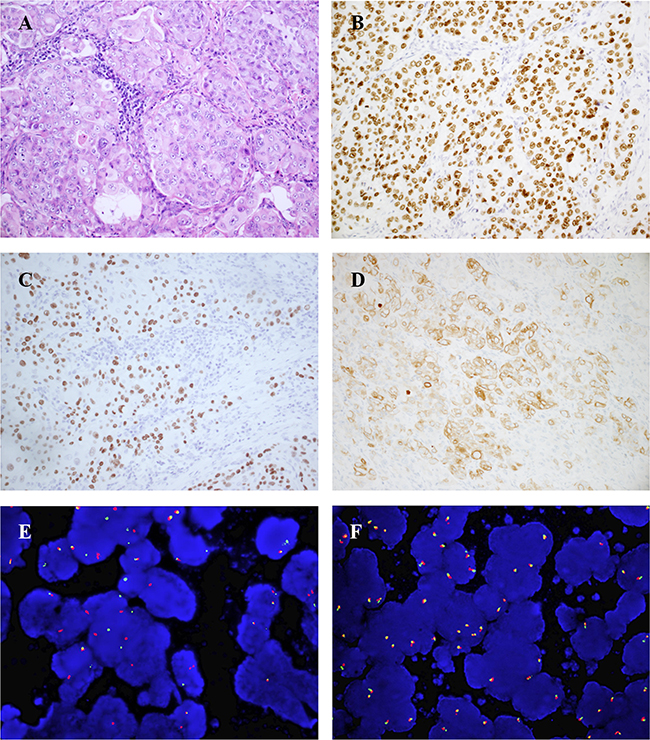
Figure 1: Representative IHC and FISH results of ROS1-rearranged advanced lung tumors (case9). (A), solid-predominant growth pattern with hepatoid tumor cells in a metastatic lung adenocarcinoma (hematoxylin and eosin, ×200). (B-D), Tumor cells diffusely co-expressed TTF-1 (B, TTF-1 immunostain, ×200), p40 (C, p40 immunostain, ×200) and CK5/6(D, CK5/6 immunostain, ×200). (E), ROS1 FISH result using break-apart probes showed ROS1 rearrangement (splitting of green 5’ and orange 3’ signals). (F), ROS1 wild type.
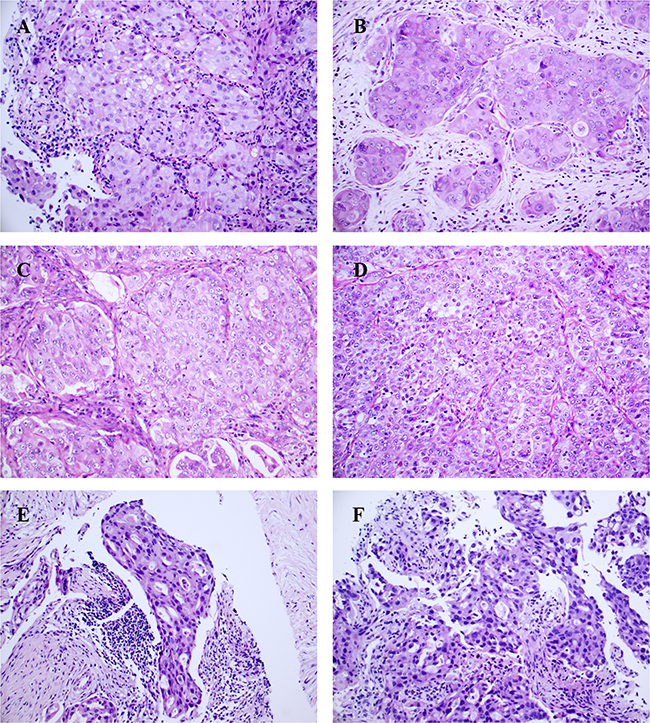
Figure 2: Representative growth patterns of ROS1-rearranged advanced lung tumors (hematoxylin and eosin, ×200): The solid-predominant growth pattern with hepatoid tumor cells in a primary lung tumor. (A) and 3 lymph node metastasis (B-D), hepatoid tumor cell shows abundant eosinophilic cytoplasm, round nuclei and prominent nucleoli; the acinar-predominant growth pattern with cribriform features in a lymph node metastasis (E) and a primary lung tumor (F).
Comparison between ROS1-positive and ROS1-negative cases
Clinical and histologic features of 16 ROS1-rearranged NSCLCs were compared with those of 122 ROS1-negative NSCLCs (Table 2). Age (P=0.001), cribriform feature (P=0.034), hepatoid cytology (P=0.016) and cytological atypia (P=0.035) were associated with ROS1- rearranged NSCLCs.
Multiple Logistic Regression Analysis
We performed multiple logistic regression analysis to identify the independent predictors for ROS1 rearrangement status. The parameters (age, hepatoid cytology, cribriform structure and cytological atypia, P < 0.1) were included in multivariate analysis. Age, hepatoid cytology and cribriform structure were identified as independent predictors for ROS1 rearrangement. The significant prediction factors for ROS1 rearrangement were shown in Table 3.
Table 3: The result of multiple logistic regression analysis
Variables |
β-Coefficient |
Wald Test |
p-Value |
OR |
95%CI |
|---|---|---|---|---|---|
Cribriform feature |
1.864 |
3.967 |
0.046 |
6.453 |
1.030-40.417 |
Hepatiod cell |
1.639 |
5.324 |
0.021 |
5.149 |
1.28-20.718 |
Age |
-0.063 |
5.391 |
0.020 |
0.939 |
0.890-0.990 |
Constant |
0.021 |
0.000 |
0.991 |
1.021 |
DISCUSSION
Our analysis of 138 advanced NSCLC cases with available clinical data and enough tissue identified age, hepatoid cytology and cribriform structure as the independent predictors for ROS1 rearrangement, which may help to find candidates for genomic alterations, especially when available tissue samples are limited.
Our study revealed that 3.7% (19 out of 516) of advanced lung adenocarcinomas harbored ROS1 rearrangement. This prevalence was a little higher than that of the entire adenocarcinoma cohort. This may due to all our patients were in IV stage. Most literature reported ROS1 rearrangement in 1-2% adenocarcinoma lung, but more than 3% in IV-stage lung adenocarcinoma. Bergethon et al screened 1,073 patients with NSCLC, 18 (1.7%) were ROS1-rearranged by FISH [15]. In IV-stage lung adenocarcinoma, 3.4% (11/327) were ROS1-rearranged. Kim et al found 3 (3.5%) of 86 IV-stage lung adenocarcinomas harbored ROS1 rearrangements [16]. What’s more, 3 cases in 98 IV-stage lung adenocarcinomas (3/98, 3.1%) were ROS1 rearrangement in the cohort of Sholl et al [17]. Many reports also found that ROS1 rearrangement was enriched in advanced group. Scheffler et al found 19 patients of 1035 (1.8%) had ROS1 rearrangement [18]. The majority of patients presented with stage IV disease at diagnosis (73.7%, 14/19). Mazieres et al identified 32 patients with ROS1 FISH-positive lung cancer in 16 centers from six European countries, and 80.7% (25/32) of these patients were IV-stage lung adenocarcinoma [19].
A correlation between histomorphology and ROS1-rearranged lung adenocarcinomas has been demonstrated in prior reports. The majority of the reports have focused on surgical specimens, but only limited studies assessed histomorphology of biopsies, which are procured frequently, especially from patients presenting at an advanced stage of disease and for whom crizotinib is recommended. To the best of our knowledge this is the largest series of ROS1-rearranged advanced cases studied to clarify the clinicopathological features. We found that ROS1-rearranged advanced lung adenocarcinomas were characterized by two growth patterns: solid growth (12/16) and acinar (4/16) growth. A lepidic pattern was absent in our series, which was similar with other studies [13, 20]. Noguchi suggested that lung adenocarcinoma develop from atypical adenomatous hyperplasia (AAH) through lepidic pattern, and finally invasive adenocarcinoma, being the solid pattern the less differentiated adenocarcinoma component [21]. Infrequent existence with lepidic pattern in ROS1-rearranged NSCLCs may lead to the hypothesis that ROS1 may be a strong oncogenic driver in NSCLCs, and the oncogenic drive of the ROS1 fusion gene might be powerful enough to bypass the lepidic phase.
The majority of ROS1-rearranged advanced lung adenocarcinomas in our series showed a solid growth pattern (75%, 12/16). Interestingly, solid pattern often possessed hepatoid cell (66.7%, 8/12), which showed abundant eosinophilic cytoplasm, round nuclei, and prominent nucleoli. This finding was in agreement with previous reports [22]. Khozin et al reported a patient with hepatoid carcinoma of the lung harbored ALK gene rearrangement [23]. Hepatoid adenocarcinomas have been defined as AFP-producing adenocarcinomas with morphologic features similar to hepatocellular carcinoma [24–26]. But 8 cases in our study were negative for antibodies Hep, AFP and Gpc3, and serum alpha-fetoprotein (AFP) were also low (0.6-2.8ng/ml). These finding suggested that these 8 cases with hepatoid cell were not hepatoid adenocarcinomas. We defined them as “poorly differentiated adenocarcinomas with solid growth pattern and eosinophilic cytoplasm”. Careful attention to this feature may lead to find the candidate of advanced NSCLC cases with ROS1 rearrangement.
Immunohistochemically, 5 of our cases co-expressed TTF-1 and p63, and 4 of them were positive for p40, and 2 cases were also positive for CK5/6. P40, an isoform of p63, has been proposed to be a specific marker of squamous cell carcinoma. In contrast with p63, the expression of p40 was more specific for squamous cell carcinoma [27]. Recent studies reported that 4 cases exhibited unequivocal squamous differentiation, co-expression for TTF1 and p63 [12, 20, 28]. Yonshida et al suggested TTF-1/p63 co-expression occurred frequently in ALK-positive NSCLCs [29]. But actually Rekhtman et al found that only 5.4% lung adenocarcinomas co-express TTF-1and p63 in general [30], even less for TTF1 and p40 co-expression. Zhao et al found that ALK, ROS1 or RET gene rearrangements appeared 0 times in 214 cases of lung squamous cancer [31], suggesting that the prevalence of ROS1 rearrangement is very low in SCC histology. We suppose that histology of ROS1+ lung cancer has low differentiation with peculiar immunoprofile, which may indicate that the cell of origin of ROS1+ lung adenocarcinoma may different from most lung adenocarcinomas.
In our series, signet-ring cells presented only in two cases (2/12), which seems lower in previous reports with surgical cases (33-55%) [12, 20], and much lower than ALK-rearranged lung adenocarcinoma (71%) [11]. Furthermore, only one case with solid growth pattern showed psammomatous calcifications, while Sholl et al found psammomatous calcifications were highly associated with ROS1 rearrangement (6 of 9 or 66%vs. 1 of 185 or 0.5%; P<0.001) as compared with ROS1 wild type [17]. These differences may be due to the differences in specimen source (lung resection vs. biopsy) and tumor stage (early vs. advanced). Some features frequently presented in lung resections may be missed because of the limited tissue samples. Thus, it is essential to find out the features of advanced lung adenocarcinoma with ROS1 rearrangement.
The results of our study highlight that hepatoid cytology and cribriform structure may be the key morphologic features associated with advanced lung adenocarcinomas with ROS1 rearrangement. The recognition of hepatoid cytology and cribriform structure could help to triage a specimen for appropriate molecular testing, especially when tissue is limited. However, the diagnosis of ROS1-rearrangement needs to be validated by FISH or real-time PCR.
MATERIALS AND METHODS
Patients and samples
The study was approved by the Ethics Committee of the First Affiliated Hospital of Zhejiang University. The Ethics Committee waived the need for consent for the use of the samples in this research study. Our study group consisted of 516 consecutive cases of IV-stage lung adenocarcinoma diagnosed at the First Affiliated Hospital of Zhejiang University between 2014 and 2016, 19 of which were ROS1+ and 497 of which were ROS1-. ROS1 rearrangements were detected using real-time PCR and FISH, as described below. The specimen types consisted of small biopsies (n=499) and cell blocks (n=13) or Ebus (n=4). The clinical characteristics of all patients are summarized in Table1. In order to clarify clinicopathological characteristics of ROS1 rearrangement, samples with available medical records and enough tumor cells for histological analysis were separated into two groups: 16 ROS1+ and 122 ROS1-. 3 ROS1-rearranged cases (1 biopsy and 2 cell blocks) have too few tumor cells to histological analysis.
Pathology review
Hematoxylin and eosin (H&E)-stained slides of all samples were reviewed by two experienced pathologists (MK and WD) to evaluate the histologic characteristics based on the 2015 WHO classification of lung adenocarcinoma [32]. Immunohistochemistry analyses for P63 (clone 7JUL, Long island bio, Shanghai, China), P40 (cloneBC28, ZSGB-BIO, Beijing, China), CK5/6 (clone D5/16B4, Long island bio, Shanghai, China), CK7 (clone OV-TL12/30, Long island bio, Shanghai, China), and TTF-1 (clone SPT24, ZSGB-BIO, Beijing, China) were performed to differentiate between adenocarcinoma and squamous cell carcinoma. Antibodies for Hep (Hepatocyte, clone OCH1E5, ZSGB-BIO, Beijing, China), AFP (clone ZSA06, ZSGB-BIO, Beijing, China) and Gpc3 (Glypican-3, clone 1G12, ZSGB-BIO, Beijing, China) were evaluated in 5 tumors with hepatoid cytology. Immunohistochemistry was performed on 4 μm-thick FFPE tissues using Ventana automated immunostainer (Ventana Medical Systems, Tucson, AZ) according to the manufacturer’s protocol. Antigen retrieving was performed with EDTA (pH9.0) for 20 minutes. Cytological atypia of tumors were classified as mild atypia (relatively uniform nuclei with indistinct nucleoli at 100 × magnification), moderate atypia (relatively uniform nuclei with distinct nucleoli at 100 × magnifications) and severe atypia (bizarre, enlarged nuclei of varied sizes, with some nuclei at least twice as large as others) [33]. The highest degree of atypia was recorded for heterogeneous tumors. Hepatoid cytology was defined as the solid pattern with hepatoid tumor appearance characterized by abundant eosinophilic cytoplasm, round and relatively monomorphic nuclei, and prominent nucleoli [11].
Fluorescence In Situ hybridization
Slices of FFPE tissues, 4μm thick, were used to evaluate the presence of ROS1 gene fusion by FISH, using a break-apart probe for ROS1 (6q22 ROS1 Break Apart FISH Probe; Abbott Molecular, Des Plaines, IL, USA). Nuclei were counterstained with DAPI (Zytovision, Bremerhaven, Germany) and slides were examined with a BX51 fluorescence microscope (Olympus, Tokyo, Japan) equipped with a triple-pass filter (DAPI/Green/Orange). Samples were considered to be ROS1 positive if more than 15% of tumor cells showed split red and green signals (signals separated by ≥1 signal diameter) or single 3’ signals. Otherwise the samples were considered as FISH negative.
Real-time PCR
ROS1 was amplified by multiplex real-time PCR using a Stratagene Mx3000P real-time PCR system (Stratagene, CA) with an AmoyDx® ROS1 fusion gene detection kit (Amoy Diagnostics Co., Ltd, Xiamen, China). All types of ROS1 gene fusions detected with the detection kit were listed in Supplementary Table S2. A case was considered positive for ROS1 rearrangement if FAM Ct value was <30. Otherwise the samples were considered as negative. The sample may contain two or more fusion patterns simultaneously. The status of the EGFR mutation and ALK rearrangement were also analyzed by real-time PCR and IHC, according to methods previously described [34].
Statistical analysis
Statistical analysis was performed using SPSS software version 17.0 (SPSS Inc., Chicago, IL). Continuous variables were analyzed using Student T test. The categorized variables were analyzed using Chi-square test. Multivariate analysis was performed to determine the discriminating power of each histologic parameter between ROS1-positive and ROS1-negative cohorts by multiple logistic regressions. P<0.05 was considered statistically significant.
ACKNOWLEDGMENTS
The authors thank Qihan You for technical assistance.
CONFLICTS OF INTEREST
There is no conflict of interest.
GRANT SUPPORT
This work was supported by grants from the Medicine and Health Project of Zhejiang Province, China (Grant No. 2015104004).
REFERENCES
1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015; 65: 87-108.
2. Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger KR, Yatabe Y, Beer DG, Powell CA, Riely GJ, Van Schil PE, Garg K, Austin JH, Asamura H et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol. 2011; 6: 244-285.
3. Paez JG, Janne PA, Lee JC, Tracy S, Greulich H, Gabriel S, Herman P, Kaye FJ, Lindeman N, Boggon TJ, Naoki K, Sasaki H, Fujii Y et al. EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy. Science. 2004; 304: 1497-1500.
4. Lynch TJ, Bell DW, Sordella R, Gurubhagavatula S, Okimoto RA, Brannigan BW, Harris PL, Haserlat SM, Supko JG, Haluska FG, Louis DN, Christiani DC, Settleman J et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med. 2004; 350: 2129-2139.
5. Kwak EL, Bang YJ, Camidge DR, Shaw AT, Solomon B, Maki RG, Ou SH, Dezube BJ, Janne PA, Costa DB, Varella-Garcia M, Kim WH, Lynch TJ et al. Anaplastic lymphoma kinase inhibition in non-small-cell lung cancer. N Engl J Med. 2010; 363: 1693-1703.
6. Stumpfova M, Janne PA. Zeroing in on ROS1 rearrangements in non-small cell lung cancer. Clin Cancer Res. 2012; 18: 4222-4224.
7. Shaw AT, Ou SH, Bang YJ, Camidge DR, Solomon BJ, Salgia R, Riely GJ, Varella-Garcia M, Shapiro GI, Costa DB, Doebele RC, Le LP, Zheng Z et al. Crizotinib in ROS1-rearranged non-small-cell lung cancer. N Engl J Med. 2014; 371: 1963-1971.
8. Boland JM, Wampfler JA, Jang JS, Wang X, Erickson-Johnson MR, Oliveira AM, Yang P, Jen J, Yi ES. Pulmonary adenocarcinoma with signet ring cell features: a comprehensive study from 3 distinct patient cohorts. Am J Surg Pathol. 2014; 38: 1681-1688.
9. Pareja F, Crapanzano JP, Mansukhani MM, Bulman WA, Saqi A. Cytomorphological features of ALK-positive lung adenocarcinomas: psammoma bodies and signet ring cells. Cancer Cytopathol. 2015; 123: 162-170.
10. Yoshida A, Tsuta K, Watanabe S, Sekine I, Fukayama M, Tsuda H, Furuta K, Shibata T. Frequent ALK rearrangement and TTF-1/p63 co-expression in lung adenocarcinoma with signet-ring cell component. Lung Cancer. 2011; 72: 309-315.
11. Nishino M, Klepeis VE, Yeap BY, Bergethon K, Morales-Oyarvide V, Dias-Santagata D, Yagi Y, Mark EJ, Iafrate AJ, Mino-Kenudson M. Histologic and cytomorphologic features of ALK-rearranged lung adenocarcinomas. Mod Pathol. 2012; 25: 1462-1472.
12. Yoshida A, Kohno T, Tsuta K, Wakai S, Arai Y, Shimada Y, Asamura H, Furuta K, Shibata T, Tsuda H. ROS1-rearranged lung cancer: a clinicopathologic and molecular study of 15 surgical cases. Am J Surg Pathol. 2013; 37: 554-562.
13. Go H, Kim DW, Kim D, Keam B, Kim TM, Lee SH, Heo DS, Bang YJ, Chung DH. Clinicopathologic analysis of ROS1-rearranged non-small-cell lung cancer and proposal of a diagnostic algorithm. J Thorac Oncol. 2013; 8: 1445-1450.
14. Seung Eun Lee BL MH, et al. Comprehensive analysis of RET and ROS1 rearrangement in lung adenocarcinoma. Modern Pathology. 2015; 28: 468–479.
15. Bergethon K, Shaw AT, Ou SH, Katayama R, Lovly CM, McDonald NT, Massion PP, Siwak-Tapp C, Gonzalez A, Fang R, Mark EJ, Batten JM, Chen H et al. ROS1 rearrangements define a unique molecular class of lung cancers. J Clin Oncol. 2012; 30: 863-870.
16. Kim HR, Lim SM, Kim HJ, Hwang SK, Park JK, Shin E, Bae MK, Ou SH, Wang J, Jewell SS, Kang DR, Soo RA, Haack H et al. The frequency and impact of ROS1 rearrangement on clinical outcomes in never smokers with lung adenocarcinoma. Ann Oncol. 2013; 24: 2364-2370.
17. Sholl LM, Sun H, Butaney M, Zhang C, Lee C, Janne PA, Rodig SJ. ROS1 immunohistochemistry for detection of ROS1-rearranged lung adenocarcinomas. Am J Surg Pathol. 2013; 37: 1441-1449.
18. Scheffler M, Schultheis A, Teixido C, Michels S, Morales-Espinosa D, Viteri S, Hartmann W, Merkelbach-Bruse S, Fischer R, Schildhaus HU, Fassunke J, Sebastian M, Serke M et al. ROS1 rearrangements in lung adenocarcinoma: prognostic impact, therapeutic options and genetic variability. Oncotarget. 2015; 6: 10577-10585. doi: 10.18632/oncotarget.3387.
19. Mazieres J, Zalcman G, Crino L, Biondani P, Barlesi F, Filleron T, Dingemans AM, Lena H, Monnet I, Rothschild SI, Cappuzzo F, Besse B, Thiberville L et al. Crizotinib therapy for advanced lung adenocarcinoma and a ROS1 rearrangement: results from the EUROS1 cohort. J Clin Oncol. 2015; 33: 992-999.
20. Mescam-Mancini L, Lantuejoul S, Moro-Sibilot D, Rouquette I, Souquet PJ, Audigier-Valette C, Sabourin JC, Decroisette C, Sakhri L, Brambilla E, McLeer-Florin A. On the relevance of a testing algorithm for the detection of ROS1-rearranged lung adenocarcinomas. Lung Cancer. 2014; 83: 168-173.
21. Noguchi M, Morikawa A, Kawasaki M, Matsuno Y, Yamada T, Hirohashi S, Kondo H, Shimosato Y. Small adenocarcinoma of the lung. Histologic characteristics and prognosis. Cancer. 1995; 75: 2844-2852.
22. Pan Y, Zhang Y, Li Y, Hu H, Wang L, Li H, Wang R, Ye T, Luo X, Zhang Y, Li B, Cai D, Shen L et al. ALK, ROS1 and RET fusions in 1139 lung adenocarcinomas: a comprehensive study of common and fusion pattern-specific clinicopathologic, histologic and cytologic features. Lung Cancer. 2014; 84: 121-126.
23. Khozin S, Roth MJ, Rajan A, Smith K, Thomas A, Berman A, Giaccone G. Hepatoid carcinoma of the lung with anaplastic lymphoma kinase gene rearrangement. J Thorac Oncol. 2012; 7: e29-31.
24. Haninger DM, Kloecker GH, Bousamra Ii M, Nowacki MR, Slone SP. Hepatoid adenocarcinoma of the lung: report of five cases and review of the literature. Mod Pathol. 2014; 27: 535-542.
25. Hayashi Y, Takanashi Y, Ohsawa H, Ishii H, Nakatani Y. Hepatoid adenocarcinoma in the lung. Lung Cancer. 2002; 38: 211-214.
26. Ishikura H, Fukasawa Y, Ogasawara K, Natori T, Tsukada Y, Aizawa M. An AFP-producing gastric carcinoma with features of hepatic differentiation. A case report. Cancer. 1985; 56: 840-848.
27. Ikeda S, Naruse K, Nagata C, Kuramochi M, Onuki T, Inagaki M, Suzuki K. Immunostaining for thyroid transcription factor 1, Napsin A, p40, and cytokeratin 5 aids in differential diagnosis of non-small cell lung carcinoma. Oncol Lett. 2015; 9: 2099-2104.
28. Cai W, Li X, Su C, Fan L, Zheng L, Fei K, Zhou C, Manegold C, Schmid-Bindert G. ROS1 fusions in Chinese patients with non-small-cell lung cancer. Ann Oncol. 2013; 24: 1822-1827.
29. Yoshida A, Tsuta K, Nakamura H, Kohno T, Takahashi F, Asamura H, Sekine I, Fukayama M, Shibata T, Furuta K, Tsuda H. Comprehensive histologic analysis of ALK-rearranged lung carcinomas. Am J Surg Pathol. 2011; 35: 1226-1234.
30. Rekhtman N, Ang DC, Sima CS, Travis WD, Moreira AL. Immunohistochemical algorithm for differentiation of lung adenocarcinoma and squamous cell carcinoma based on large series of whole-tissue sections with validation in small specimens. Mod Pathol. 2011; 24: 1348-1359.
31. Zhao W, Choi YL, Song JY, Zhu Y, Xu Q, Zhang F, Jiang L, Cheng J, Zheng G, Mao M. ALK, ROS1 and RET rearrangements in lung squamous cell carcinoma are very rare. Lung Cancer. 2016; 94: 22-27.
32. Travis WD, Brambilla E, Burke AP, Marx A, Nicholson AG. WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart. Fourth edition. International Agency for Research on Cancer, Lyon, France (2015).
33. von der Thusen JH, Tham YS, Pattenden H, Rice A, Dusmet M, Lim E, Nicholson AG. Prognostic significance of predominant histologic pattern and nuclear grade in resected adenocarcinoma of the lung: potential parameters for a grading system. J Thorac Oncol. 2013; 8: 37-44.
34. Zhou JY, Zhao J, Sun K, Wang B, Wang LJ, Chen X, Zheng J, You QH, Wang XL, Ding W, Zhou JY. Accurate and Economical Detection of ALK Positive Lung Adenocarcinoma with Semiquantitative Immunohistochemical Screening. Plos One. 2014; 9.