
INTRODUCTION
Renal cell carcinomas (RCC) comprises 2-3% of all non-cutaneous malignant neoplasms in adults of both genders [1]. There are estimated 63,920 new cases and 13,860 deaths from renal cancer in the United States in 2014 [2]. Renal epithelial tumors arise from renal tubules and use to be classified into 4 major categories based on morphology, they are, clear cell renal carcinomas (ccRCCs) (75%), papillary renal carcinomas (PRCCs) (15%), chromophobe renal cell carcinoma (chRCC) (5%), and oncocytomas (5%) [3]. In the 2004, the World Health Organization (WHO) classified renal-tumor oncocytomas as benign neoplasms, the reported incidence rate of oncocytomas varies from 3.2% to 7%[4]. Accurate distinction between renal cell carcinomas and renal oncocytomas have significant prognostic.
CKs are a class of intermediate filaments that are the basic markers of epithelial differentiation[5]. They consist of at least 20 distinct molecules, the expression of which depends on cell type and differentiation position, making them useful in differential diagnosis of many epithelial tumors[5].
CK7 are increased expressed in a variety of RCC but show a more restricted expression in normal tissues or benign neoplasms [5–7]. CK7 was helpful in several diagnostic RCC [8], [9], and a useful marker in the differential diagnosis of epithelial tumors., evaluation of CK7 as new markers of differentiating RCC (ccRCCs, PRCCs and chRCC) from Oncocytomas is needed.
In an attempt to confirm the potential role of CK7 expression as a prognostic biomarker, we completed a meta-analysis of CK7 expression in patient of Asia and European lineage across different geographic regions with RCC and Oncocytomas.
Meta-analysis results
When we pooled 21 eligible studies into the meta-analysis, result revealed that positive CK7 by IHC was significantly associated with increased diagnosis of RCC than Oncocytomas (OR=10.64; 95% CI, 7.44-15.23; P=0.0001) (Figure 2). Funnel plot asymmetry couldn’t be observed (Figure 3), which suggested no evidence publication bias existing.
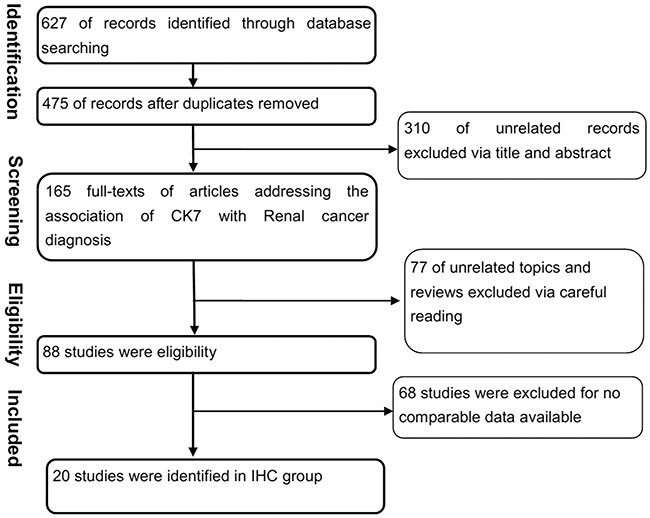
Figure 1: Flowchart of selecting process for meta-analysis. A total of 628 articles were assembled. After full review, 21 articles were included.
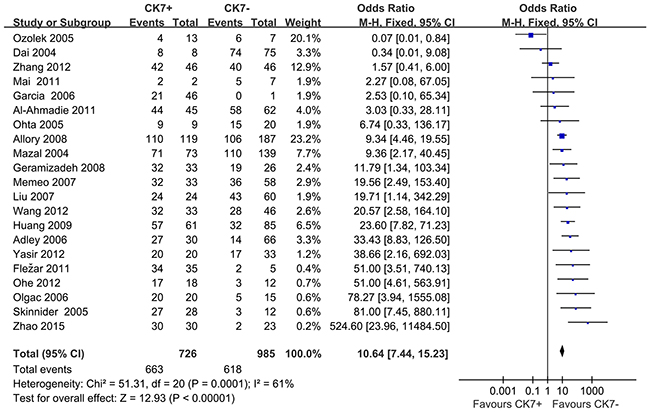
Figure 2: Forest plots for overall analysis of association of positive CK7 by immunohistochemistry with RCC and Oncocytomas, under random-effects model. M-H=Mantel-Haenszel method; CI=confidence interval.
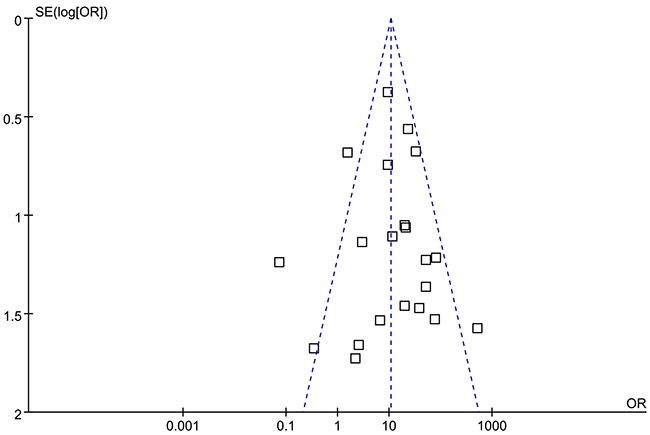
Figure 3: Funnel plots illustrating meta-analysis of overall analysis. SE = standard error; OR = odds ratio.
In consideration of the potential different expression of CK7 in different races, we yielded ethnicity-based subgroup-analyses (Figure 4). Subgroup-analysis showed that findings didn’t substantially change when only Caucasians (OR=10.58; 95% CI, 6.97-16.07; P=0.002), or Asians were included (OR=10.83; 95% CI, 5.39-21.74; P=0.004). Both the results of subgroup-analyses showed that heterogeneity was usually a variation affecting the degree of risk rather than direction of effect.
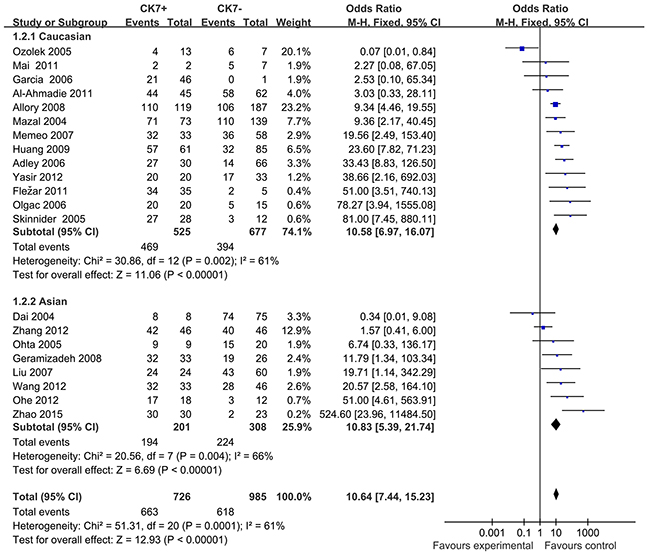
Figure 4: Forest plots for subgroup-analysis of association of positive CK7 by immunohistochemistry associated with RCC and Oncocytomas in Caucasians and Asians. M-H=Mantel-Haenszel method; CI=confidence interval.
DISCUSSION
In this study, we explored the possible role of CK7 in distinguishing RCC from Renal Oncocytomas in 21 studies from various geographic regions including European and Asia[10–31]. CK7 expression by IHC was significantly associated with increased diagnosis of RCC (OR=10.64; 95% CI, 7.44-15.23; P=0.0001). The overall-analysis provided strong replication of the initial findings, confirming the CK7 for RCC.
All cases in our report followed the World Health Organization classification of renal tumors as standard level, based on a constellation of histologic features. It is difficult to make a correct histological diagnosis of RCC and Renal Oncocytomas based only on conventional routine staining, due to overlapping morphological characteristics[32–35]. Many researchers worked hard to find a way to differentiate RCC from Renal Oncocytomas. Some investigators have unsuccessfully reported that colloidal iron staining is not specific for distinguishing RCC from Oncocytomas[36,37]. But Ancillary methods, including histochemical and immunohistochemical stains, have been shown to be useful in the differential diagnosis of renal neoplasms. We summarized CK7 staining in the majority of RCC diffusely expressing membranous and Oncocytoma being typically negative or, at most, focally positive in scattered cells[12,14,18]. Matthewreported that CK7 is helper for diagnosis in circulating tumor cells (CTCs) of tissue of origin in breast cancer , prostate cancer and more expression in gastrointestinal, respiratory and gynecological malignancies[38,39,40]. Kinney proved that CK7 differentiate from Metanephric adenoma and papillary renal cell carcinoma[41]. Few researcher reported CK7 is more expression in Oncocytomas than in RCC[10,11]. In our approach we evaluated the potential diagnostic use of the expression of CK7 distinguishing RCC from Renal Oncocytomas in 21 studies(OR=10.64; 95% CI, 7.44-15.23; P=0.0001). The meta-analysis is a method that can solve the problem created by low statistical power in a single study to draw a more robust conclusion than the body of evidence. Our findings suggest that Ck7 may increase RCC diagnosis in the future.
Strengths of this study include its large sample size. Because of this, the geographic regions were distinguished in subgroup-analyses. However, our results are based on unadjusted estimates.
CONCLUSION
Meta-analysis of the comprehensive literature revealed that the CK7 expression was strongly associated with RCC risk from various regions. CK7 is helpful in distinguishing RCC from Oncocytomas. There was no varying between Caucasian and Asia man.
Evidence acquisition
Search strategy and selection criteria
We carried out a comprehensive literature review with search terms (Table 1). A comprehensive and systematic search through Medline, Web of Science and the Cochrane Library. The last quest was updated on May 25, 2015. When more than one studies with the same population were identified, only the most recent or complete one was included in this meta-analysis.
Table 1: Characteristics of trials included in meta-analyses
Study |
Year |
methods |
Ethnicity |
Cases |
Controls |
Study design |
Control source |
||
|---|---|---|---|---|---|---|---|---|---|
Postive |
total |
Postive |
total |
||||||
Memeo [14] |
2007 |
IHC |
Caucasian |
32 |
68 |
1 |
23 |
cohort |
Oncocytomas |
Garcia [15] |
2006 |
IHC |
Caucasian |
21 |
21 |
25 |
26 |
cohort |
Oncocytomas |
Skinnider [16] |
2005 |
IHC |
Caucasian |
27 |
30 |
1 |
10 |
cohort |
Oncocytomas |
Al-Ahmadie [17] |
2011 |
IHC |
Caucasian |
44 |
102 |
1 |
5 |
cohort |
Oncocytomas |
Huang [18] |
2009 |
IHC |
Caucasian |
57 |
89 |
4 |
57 |
cohort |
Oncocytomas |
Mai [19] |
2011 |
IHC |
Caucasian |
2 |
7 |
0 |
2 |
cohort |
Oncocytomas |
Yasir [20] |
2012 |
IHC |
Caucasian |
20 |
37 |
0 |
16 |
cohort |
Oncocytomas |
Olgac [21] |
2006 |
IHC |
Caucasian |
20 |
25 |
0 |
10 |
cohort |
Oncocytomas |
Allory [22] |
2008 |
IHC |
Caucasian |
110 |
216 |
9 |
90 |
cohort |
Oncocytomas |
Fležar [23] |
2011 |
IHC |
Caucasian |
34 |
36 |
1 |
4 |
cohort |
Oncocytomas |
Mazal [24] |
2004 |
IHC |
Caucasian |
71 |
73 |
110 |
139 |
cohort |
Oncocytomas |
Skinnider [25] |
2005 |
IHC |
Caucasian |
27 |
45 |
1 |
10 |
cohort |
Oncocytomas |
Ozolek [26] |
2005 |
IHC |
Caucasian |
4 |
10 |
9 |
10 |
cohort |
Oncocytomas |
Adley [27] |
2006 |
IHC |
Caucasian |
27 |
41 |
3 |
55 |
cohort |
Oncocytomas |
Liu [28] |
2007 |
IHC |
Asia |
24 |
67 |
0 |
17 |
cohort |
Oncocytomasl |
Ohta [29] |
2005 |
IHC |
Asia |
9 |
24 |
0 |
5 |
cohort |
Oncocytomas |
Ohe [30] |
2012 |
IHC |
Asia |
17 |
20 |
1 |
10 |
cohort |
Oncocytomas |
Wang [31] |
2012 |
IHC |
Asia |
32 |
60 |
1 |
19 |
cohort |
Oncocytomas |
Zhang Z [32] |
2012 |
IHC |
Asia |
42 |
82 |
4 |
10 |
cohort |
Oncocytomas |
Dai [33] |
2004 |
IHC |
Asia |
8 |
82 |
0 |
1 |
cohort |
Oncocytomas |
Zhao [30] |
2015 |
IHC |
Asia |
30 |
32 |
0 |
21 |
cohort |
Oncocytomas |
Geramizadeh [31] |
2008 |
IHC |
Asia |
32 |
51 |
1 |
8 |
cohort |
Oncocytomas |
IHC=Immunohistochemistry;
Studies were included if they fulfilled the following criteria: 1) studies that included the pathologically confirmed diagnosis of RCC, 2) the control group consisted of subjects who were the pathologically confirmed diagnosis of Oncocytomas , 3) studies that offered a hazard ratio (HR) and 95% confidence interval (CI) categorically or the data presented were available for calculation of the HR and 95% CI.
Data extraction and quality assessment
This meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [42] and Meta-analysis of Observational Studies in Epidemiology (MOOSE) [43] guidelines.
Study ethnicity of included subjects, numbers of cases and control subjects, and positive staining were extracted for factors of interest. The authors of published studies were also contacted for requesting necessary data that were not provided. Quality assessment was undertaken independently by at least four authors (Ning Jiang, Fuling Ma, Liang Dai, Zhun Wang). Two authors (Liqun Zhou, Yuanjie Niu) independently did the literature search and carefully extracted data. Any disagreements were resolved through discussion with authors (Niu and Jiang).
Data analysis and presentation
We used the crude odds radio (OR) with their corresponding 95 % confidence intervals (CI) as the metric of choice. The random effects model of DerSimonian and Laird was prespecified for use in all estimates because of the suspected a priori that studies were conducted by various authors with different populations and had different designs (eg, case-control and case series studies). Heterogeneity was evaluated using the Q test [44]. We also calculated the quantity I2 statistic that represented the percentage of total variation across studies. As a guide, (I2=0–25 %: no heterogeneity; I2=25–50 %: moderate heterogeneity; I2=50–75 %: large heterogeneity; I2=75–100 %: extreme heterogeneity) [45]. The funnel plot was addressed to reveal the potential publication bias. All analyses were conducted using Review Manage, version 5.2 (The Cochrane Collaboration, Oxford, U.K.).
Evidence synthesis
Literature search and characteristics of studies
Initially, we assembled a total of 629 articles. After review of the abstracts, 166 studies were identified as potentially eligible for inclusion. After full review, 21 studies [10–31] using immunohistochemical method (IHC) were deemed eligible and were included in the study. The list of studies excluded and reasons for exclusion are shown in Figure 1.
The included studies were published from 2004 to 2015. Six conducted in Asia, the others in western countries. Most of included studies chose Oncocytomas. The details were listed in Table 1.
ACKNOWLEDGMENTS
The project was supported by a research grant of National Basic Research Program of China (973 Program, 2012CB518304). and the Science Foundation of Tianjin (No.: 11JCZDJC19700) and 09ZCZDSF04300, 14KG135, 20140117 and the National Natural Science Foundation of China Grant numbers: 2012DFG32220 and 81572538, 81472682. Ph.D Programs Foundation of Ministry of Education of China 20131202110008.
REFERENCES
1. Henrique R, Luís AS, Jerónimo C. The epigenetics of renal cell tumors: from biology to biomarkers. Front Genet. 2012. 30;3:94.
2. Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64:9-29.
3. Linehan WM, Zbar B. Focus on kidney cancer. Cancer Cell. 2004;6:223-8.
4. Romis L, Cindolo L, Patard JJ, Messina G, Altieri V, Salomon L, Abbou CC, Chopin D, Lobel B, de La Taille A. Frequency, clinical presentation and evolution of renal oncocytomas: multicentric experience from a European database. Eur Urol. 2004;45:53-7.
5. Chu PG, Weiss LM. Keratin expression in human tissues and neoplasms. Histopathology. 2002;40:403-39.
6. Chu P, Wu E, Weiss LM. Cytokeratin 7 and cytokeratin 20 expression in epithelial neoplasms: a survey of 435 cases. Mod Pathol. 2000;13:962-72.
7. Adisa JO, Egbujo EC, Ibrahim B, Musa B, Madukwe J. Expression of some selected cytokeratins and Ki67 protein in prostatic tumor: can these be used as tumor markers. Pan Afr Med J. 2015;20:46.
8. Aron M, Chang E, Herrera L, Hes O, Hirsch MS, Comperat E, Camparo P, Rao P, Picken M, Michal M, Montironi R, Tamboli P, Monzon F, Amin MB. Clear cell-papillary renal cell carcinoma of the kidney not associated with end-stage renal disease: clinicopathologic correlation with expanded immunophenotypic and molecular characterization of a large cohort with emphasis on relationship with renal angiomyoadenomatous tumor. Am J Surg Pathol. 2015;39:873-88.
9. Yang P, Cornejo KM, Sadow PM, Cheng L, Wang M, Xiao Y, Jiang Z, Oliva E, Jozwiak S, Nussbaum RL, Feldman AS, Paul E, Thiele EA, et al. Renal cell carcinoma in tuberous sclerosis complex. Am J Surg Pathol. 2014;38:895-909.
10. Garcia E, Li M. Caveolin-1 immunohistochemical analysis in differentiating chromophobe renal cell carcinoma from renal oncocytoma. Am J Clin Pathol. 2006;125:392-8.
11. Ozolek JA, Bastacky SI, Myers EN, Hunt JL. Immunophenotypic comparison of salivary gland oncocytoma and metastatic renal cell carcinoma. Laryngoscope. 2005;115:1097-100.
12. Memeo L, Jhang J, Assaad AM, McKiernan JM, Murty VV, Hibshoosh H, Tong GX, Mansukhani MM. Immunohistochemical analysis for cytokeratin 7, KIT, and PAX2: value in the differential diagnosis of chromophobe cell carcinoma. Am J Clin Pathol. 2007;127:225-9.
13. Skinnider BF, Folpe AL, Hennigar RA, Lim SD, Cohen C, Tamboli P, Young A, de Peralta-Venturina M, Amin MB. Distribution of cytokeratins and vimentin in adult renal neoplasms and normal renal tissue: potential utility of a cytokeratin antibody panel in the differential diagnosis of renal tumors. Am J Surg Pathol. 2005;29:747-54.
14. Al-Ahmadie HA, Alden D, Fine SW, Gopalan A, Touijer KA, Russo P, Reuter VE, Tickoo SK. Role of immunohistochemistry in the evaluation of needle core biopsies in adult renal cortical tumors: an ex vivo study. Am J Surg Pathol. 2011;35:949-61.
15. Huang W, Kanehira K, Drew S, Pier T. Oncocytoma can be differentiated from its renal cell carcinoma mimics by a panel of markers: an automated tissue microarray study. Appl Immunohistochem Mol Morphol. 2009;17:12-7.
16. Mai KT, Ahmed I, Levac J, Nguyen BN. Fluorescent In-situ Hybridization Study of Non-papillary Oncocytic/Eosinophilic Renal Cell Carcinoma. Appl Immunohistochem Mol Morphol. 2011;19:82-91.
17. Yasir S, Herrera L, Gomez-Fernandez C, Reis IM, Umar S, Leveillee R, Kava B, Jorda M. CD10+ and CK7/RON- immunophenotype distinguishes renal cell carcinoma, conventional type with eosinophilic morphology from its mimickers. Appl Immunohistochem Mol Morphol. 2012;20:454-61.
18. Olgac S, Hutchinson B, Tickoo SK, Reuter VE. Alpha-methylacyl-CoA racemase as a marker in the differential diagnosis of metanephric adenoma. Mod Pathol. 2006;19:218-24.
19. Allory Y, Bazille C, Vieillefond A, Molinié V, Cochand-Priollet B, Cussenot O, Callard P, Sibony M. Profiling and classification tree applied to renal epithelial tumours. Histopathology. 2008;52:158-66.
20. Strojan Fležar M, Gutnik H, Jeruc J, Kirbiš IS. Typing of renal tumors by morphological and immunocytochemical evaluation of fine needle aspirates. Virchows Arch. 2011;459:607-14.
21. Mazal PR, Exner M, Haitel A, Krieger S, Thomson RB, Aronson PS, Susani M. Expression of kidney-specific cadherin distinguishes chromophobe renal cell carcinoma from renal oncocytoma. Hum Pathol. 2005;36:22-8.
22. Skinnider BF, Folpe AL, Hennigar RA, Lim SD, Cohen C, Tamboli P, Young A, de Peralta-Venturina M, Amin MB. Distribution of cytokeratins and vimentin in adult renal neoplasms and normal renal tissue: potential utility of a cytokeratin antibody panel in the differential diagnosis of renal tumors. Am J Surg Pathol. 2005;29:747-54.
23. Adley BP, Papavero V, Sugimura J, Teh BT, Yang XJ. Diagnostic value of cytokeratin 7 and parvalbumin in differentiating chromophobe renal cell carcinoma from renal oncocytoma. Anal Quant Cytol Histol. 2006;28:228-36.
24. Liu L, Qian J, Singh H, Meiers I, Zhou X, Bostwick DG. Immunohistochemical analysis of chromophobe renal cell carcinoma, renal oncocytoma, and clear cell carcinoma: an optimal and practical panel for differential diagnosis. Arch Pathol Lab Med. 2007;131:1290-7.
25. Ohta Y, Suzuki T, Shiokawa A, Mitsuya T, Ota H. Expression of CD10 and cytokeratins in ovarian and renal clear cell carcinoma. Int J Gynecol Pathol. 2005;24:239-45.
26. Ohe C, Kuroda N, Takasu K, Senzaki H, Shikata N, Yamaguchi T, Miyasaka C, Nakano Y, Sakaida N, Uemura Y. Utility of immunohistochemical analysis of KAI1, epithelial-specific antigen, and epithelial-related antigen for distinction of chromophobe renal cell carcinoma, an eosinophilic variant from renal oncocytoma. Med Mol Morphol. 2012;45:98-104.
27. Wang CC, Mao TL, Yang WC, Jeng YM. Underexpression of hepatocyte nuclear factor-1β in chromophobe renal cell carcinoma. Histopathology. 2013;62:589-94.
28. Zhang W, Yu WJ, Jiang YX, Li YJ, Han F, Liu Y, Han ZL. Chromophobe renal cell carcinoma: a clinicopathologic study and immunophenotypes of 42 cases. [Article in Chinese]. Zhonghua Bing Li Xue Za Zhi. 2012;41:76-80.
29. Dai L, Lü XH, Li ZH, Li R, Liu H, Liu YL, Hui YZ. Value of special stains and immunohistochemistry in the diagnosis of renal epithelial neoplasms. [Article in Chinese]. Zhonghua Bing Li Xue Za Zhi. 2004;33:140-2.
30. Zhao W, Tian B, Wu C, Peng Y, Wang H, Gu WL, Gao FH. DOG1, cyclin D1, CK7, CD117 and vimentin are useful immunohistochemical markers in distinguishing chromophobe renal cell carcinoma from clear cell renal cell carcinoma and renal oncocytoma. Pathol Res Pract. 2015;211:303-7.
31. Geramizadeh B, Ravanshad M, Rahsaz M. Useful markers for differential diagnosis of oncocytoma, chromophobe renal cell carcinoma and conventional renal cell carcinoma. Indian J Pathol Microbiol. 2008;51:167-71.
32. Khoury JD, Abrahams NA, Levin HS, MacLennan GT. The utility of epithelial membrane antigen and vimentin in the diagnosis of chromophobe renal cell carcinoma. Ann Diagn Pathol. 2002;6:154-8.
33. Kim MK, Kim S. Immunohistochemical profile of common epithelial neoplasms arising in the kidney. Appl Immunohistochem Mol Morphol. 2002;10:332-8.
34. Koller A, Kain R, Haitel A, Mazal PR, Asboth F, Susani M. Renal oncocytoma with prominent intracytoplasmic vacuoles of mitochondrial origin. Histopathology. 2000;37:264-8.
35. Perez-Ordonez B, Hamed G, Campbell S, Erlandson RA, Russo P, Gaudin PB, Reuter VE. Renal oncocytoma: a clinicopathologic study of 70 cases. Am J Surg Pathol. 1997;21:871-83.
36. Kuroda N, Toi M, Yamamoto M, Miyazaki E, Hayashi Y, Hiroi M, Shuin T, Enzan H. Immunohistochemical identification of intracytoplasmic lumens by cytokeratin typing may differentiate renal oncocytomas from chromophobe renal cell carcinomas. Histol Histopathol. 2004;19:23-8.
37. Tickoo SK, Amin MB, Zarbo RJ. Colloidal iron staining in renal epithelial neoplasms, including chromophobe renal cell carcinoma: emphasis on technique and patterns of staining. Am J Surg Pathol. 1998;22:419-24.
38. Matthew EM, Zhou L, Yang Z, Dicker DT, Holder SL, Lim B, Harouaka R, Zheng SY, Drabick JJ, Lamparella NE, Truica CI, El-Deiry WS. A multiplexed marker-based algorithm for diagnosis of carcinoma of unknown primary using circulating tumor cells. Oncotarget. 2016;7:3662-76. doi: 10.18632/oncotarget.6657.
39. Massard C, Loriot Y, Fizazi K. Carcinomas of an unknown primary origin--diagnosis and treatment. Nat Rev Clin Oncol. 2011;8:701-10.
40. Hua X, Huang X, Liao Z, Xian Q, Yu L. Clinicopathological and EBV analysis of respiratory epithelial adenomatoid hamartoma. Diagn Pathol. 2014;9:70.
41. Kinney SN, Eble JN, Hes O, Williamson SR, Grignon DJ, Wang M, Zhang S, Baldrige LA, Martignoni G, Brunelli M, Wang L, Comperat E, Fan R, Montironi R, MacLennan GT, Cheng L. Metanephric adenoma: the utility of immunohistochemical and cytogenetic analyses in differential diagnosis, including solid variant papillary renal cell carcinoma and epithelial-predominant nephroblastoma. Mod Pathol. 2015;28:1236-48.
42. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097.
43. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, Moher D, Becker BJ, Sipe TA, Thacker SB. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA. 2000; 283:2008-12.
44. Handoll HH. Systematic reviews on rehabilitation interventions. Arch Phys Med Rehabil. 2006;87:875.
45. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557-60.